

Clinical effectiveness and safety of olaparib in BRCA-mutated, HER2-negative metastatic breast cancer in a real-world setting: final analysis of LUCY
- PMID: 38112922
- PMCID: PMC10948524
- DOI: 10.1007/s10549-023-07165-x
Clinical effectiveness and safety of olaparib in BRCA-mutated, HER2-negative metastatic breast cancer in a real-world setting: final analysis of LUCY
Abstract
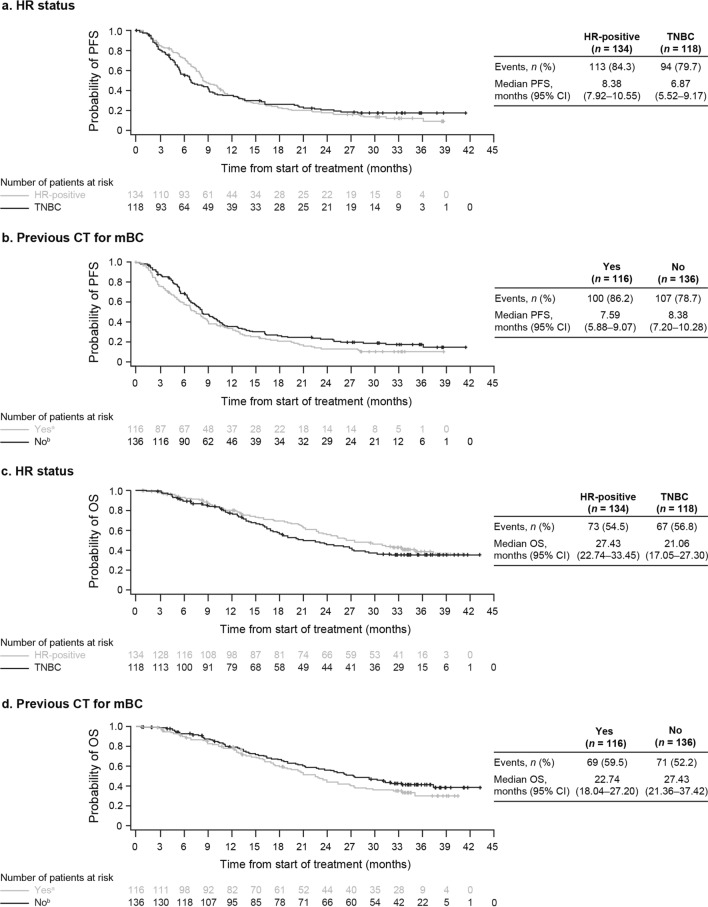
Purpose: The interim analysis of the phase IIIb LUCY trial demonstrated the clinical effectiveness of olaparib in patients with germline BRCA-mutated (gBRCAm), human epidermal growth factor receptor 2 (HER2)-negative metastatic breast cancer (mBC), with median progression-free survival (PFS) of 8.11 months, which was similar to that in the olaparib arm of the phase III OlympiAD trial (7.03 months). This prespecified analysis provides final overall survival (OS) and safety data.
Methods: The open-label, single-arm LUCY trial of olaparib (300 mg, twice daily) enrolled adults with gBRCAm or somatic BRCA-mutated (sBRCAm), HER2-negative mBC. Patients had previously received a taxane or anthracycline for neoadjuvant/adjuvant or metastatic disease and up to two lines of chemotherapy for mBC.
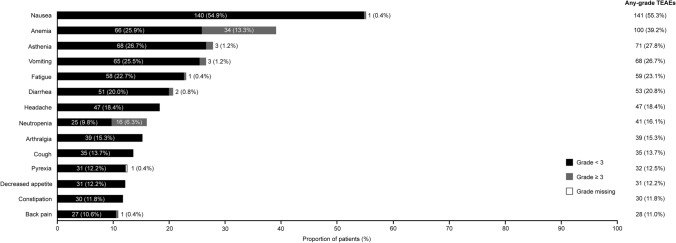
Results: Of 563 patients screened, 256 (gBRCAm, n = 253; sBRCAm, n = 3) were enrolled. In the gBRCAm cohort, median investigator-assessed PFS (primary endpoint) was 8.18 months and median OS was 24.94 months. Olaparib was clinically effective in all prespecified subgroups: hormone receptor status, previous chemotherapy for mBC, previous platinum-based chemotherapy (including by line of therapy), and previous cyclin-dependent kinase 4/6 inhibitor use. The most frequent treatment-emergent adverse events (TEAEs) were nausea (55.3%) and anemia (39.2%). Few patients (6.3%) discontinued olaparib owing to a TEAE. No deaths associated with AEs occurred during the study treatment or 30-day follow-up.
Conclusion: The LUCY patient population reflects a real-world population in line with the licensed indication of olaparib in mBC. These findings support the clinical effectiveness and safety of olaparib in patients with gBRCAm, HER2-negative mBC.
Clinical trial registration: Clinical trials registration number: NCT03286842.
Keywords: Breast cancer; Breast cancer 1 gene product; Breast cancer 2 gene product; Kaplan–Meier survival curves; Olaparib; Overall survival; Progression-free survival.
© 2023. The Author(s).
Conflict of interest statement
The following authors have received compensation for serving as a consultant, invited speaker, or medical writer, or they or the institutions they work for have received research support from the companies or organizations indicated: J Balmaña (AstraZeneca, PharmaMar, and Pfizer); PA Fasching (Agendia, Amgen, AstraZeneca, Daiichi Sankyo, Eisai, Eli Lilly, Hexal, Merck Sharp & Dohme, Novartis, Pfizer, Pierre Fabre, Roche, and Seagen); FJ Couch (Ambry Genetics, AstraZeneca, GRAIL, Qiagen, and US Oncology); S Delaloge (AstraZeneca, Besins Healthcare, Bristol Myers Squibb, Cellectis, Eli Lilly, Exact Sciences, GE, Novartis, Orion, Pfizer, Pierre Fabre, Puma Biotechnology, Rappta Therapeutics, Roche Genentech, Sanofi, Seagen, Servier, and Taiho Pharma); I Labidi-Galy (AstraZeneca and PharmaMar); J O’Shaughnessy (AbbVie, Agendia, Amgen, AstraZeneca, Bristol Myers Squibb, Celgene, Daiichi Sankyo, Eisai, Genentech, Genomic Health, GRAIL, HERON, Immunomedics, Ipsen, Jounce Therapeutics, Lilly, Merck Sharp & Dohme, Myriad Pharmaceuticals, Novartis, Odonate Therapeutics, Pfizer, Puma Biotechnology, Roche, Samsung, Sanofi, Seattle Genetics, and Syndax); YH Park (AstraZeneca, Daiichi Sankyo, Merck Sharp & Dohme, Novartis, Pfizer, and Roche); B You (AstraZeneca); H Bourgeois (Daiichi Sankyo, Lilly, and Novartis); A Goncalves (AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Merck Sharp & Dohme, Novartis, Roche, Sanofi, and Seagen); Z Kemp (AstraZeneca and Lilly); JH Sohn (AstraZeneca, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, GlaxoSmithKline, Merck Sharp & Dohme, Novartis, Pfizer, Roche, and Sanofi); S Aksoy (AstraZeneca, Bristol Myers Squibb, Eli Lilly, Merck Sharp & Dohme, Novartis, Pfizer, and Roche); CV Timcheva (AstraZeneca, Eli Lilly, i3 Research, Merck Sharp & Dohme, Novartis, Parexel, and Roche); T-W Park-Simon (AstraZeneca, Daiichi Sankyo, Eli Lilly, Exact Sciences, Gilead Sciences, GlaxoSmithKline, Merck Sharp & Dohme, Novartis, Pfizer, Roche, and Seagen); A Antón-Torres (AstraZeneca, Eli Lilly, Daichi Sankyo, Gilead, Roche, and Seagen); KA Gelmon (AstraZeneca, Ayala, Bristol Myers Squibb, Eli Lilly, Gilead Sciences, Merck Sharp & Dohme, Novartis, Pfizer, Roche, and Seagen). E John, K Baria, and I Gibson are employees and/or stockholders of AstraZeneca. T Jankowski, G Mukhametshina, E Poddubskaya, AF Eisen, and A Swampillai have declared no conflicts of interest.
Figures

References
-
- Collins JM, Nordstrom BL, McLaurin KK, Dalvi TB, McCutcheon SC, Bennett JC, et al. A real-world evidence study of CDK4/6 inhibitor treatment patterns and outcomes in metastatic breast cancer by germline BRCA mutation status. Oncol Ther. 2021;9(2):575–589. doi: 10.1007/s40487-021-00162-4. - DOI - PMC - PubMed
-
- O’Shaughnessy J, Brezden-Masley C, Cazzaniga M, Dalvi T, Walker G, Bennett J, et al. Prevalence of germline BRCA mutations in HER2-negative metastatic breast cancer: global results from the real-world, observational BREAKOUT study. Breast Cancer Res. 2020;22(1):114. doi: 10.1186/s13058-020-01349-9. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
