

Spatially Resolved Tumor Microenvironment Predicts Treatment Outcomes in Relapsed/Refractory Hodgkin Lymphoma
- PMID: 38113419
- PMCID: PMC10950131
- DOI: 10.1200/JCO.23.01115
Spatially Resolved Tumor Microenvironment Predicts Treatment Outcomes in Relapsed/Refractory Hodgkin Lymphoma
Abstract
Purpose: About a third of patients with relapsed or refractory classic Hodgkin lymphoma (r/r CHL) succumb to their disease after high-dose chemotherapy followed by autologous stem-cell transplantation (HDC/ASCT). Here, we aimed to describe spatially resolved tumor microenvironment (TME) ecosystems to establish novel biomarkers associated with treatment failure in r/r CHL.
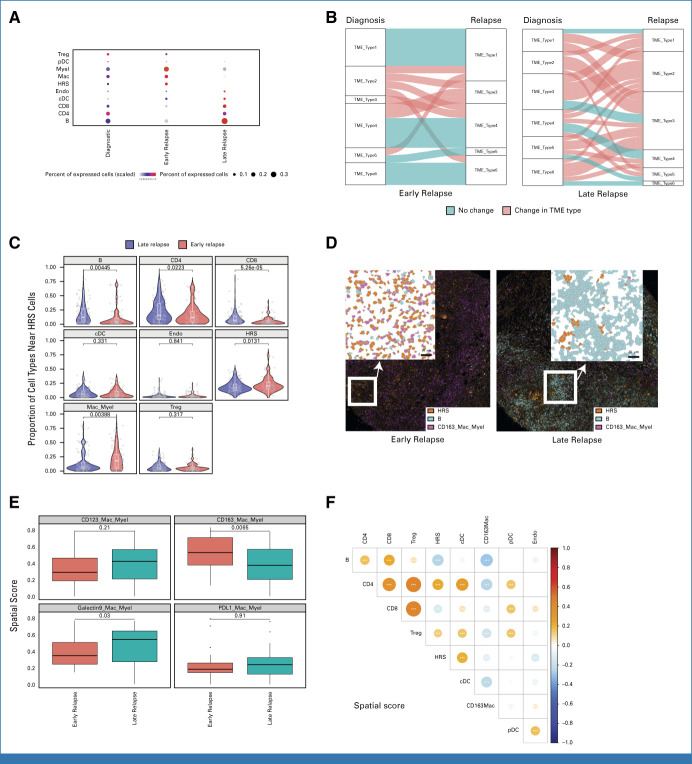
Patients and methods: We performed imaging mass cytometry (IMC) on 71 paired primary diagnostic and relapse biopsies using a marker panel specific to CHL biology. For each cell type in the TME, we calculated a spatial score measuring the distance of nearest neighbor cells to the malignant Hodgkin Reed Sternberg cells within the close interaction range. Spatial scores were used as features in prognostic model development for post-ASCT outcomes.
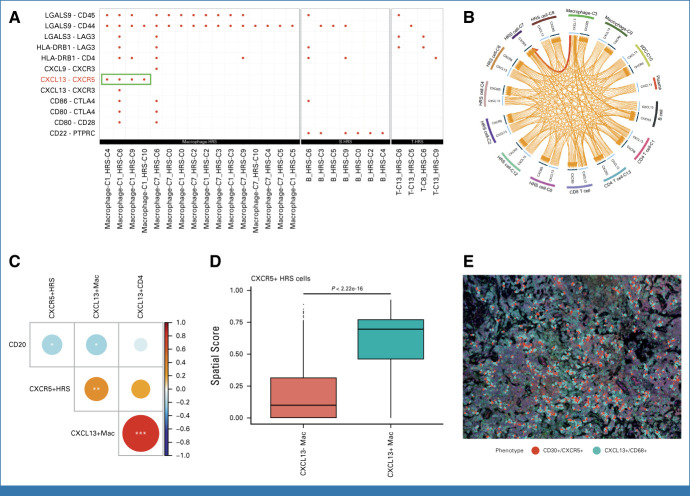
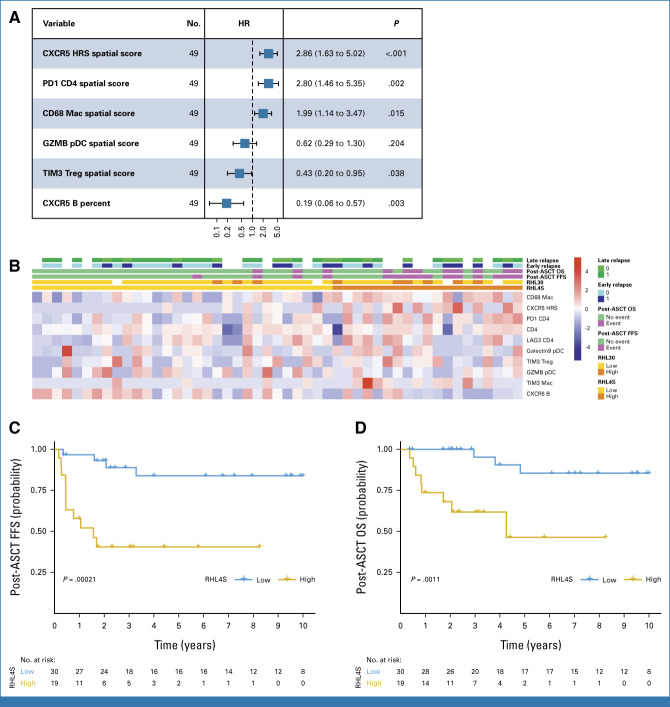
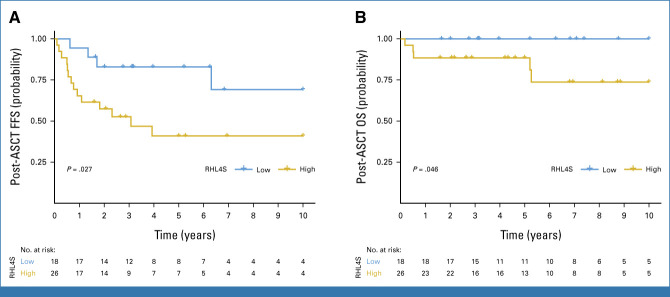
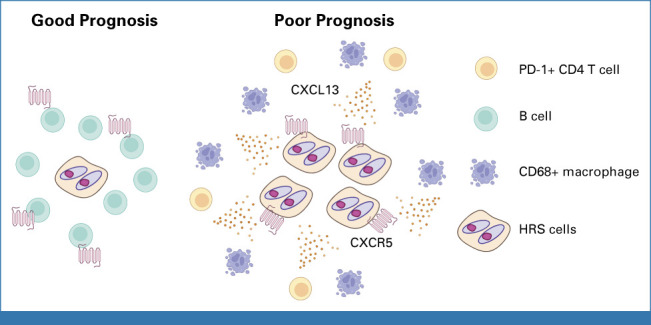
Results: Highly multiplexed IMC data revealed shared TME patterns in paired diagnostic and early r/r CHL samples, whereas TME patterns were more divergent in pairs of diagnostic and late relapse samples. Integrated analysis of IMC and single-cell RNA sequencing data identified unique architecture defined by CXCR5+ Hodgkin and Reed Sternberg (HRS) cells and their strong spatial relationship with CXCL13+ macrophages in the TME. We developed a prognostic assay (RHL4S) using four spatially resolved parameters, CXCR5+ HRS cells, PD1+CD4+ T cells, CD68+ tumor-associated macrophages, and CXCR5+ B cells, which effectively separated patients into high-risk versus low-risk groups with significantly different post-ASCT outcomes. The RHL4S assay was validated in an independent r/r CHL cohort using a multicolor immunofluorescence assay.
Conclusion: We identified the interaction of CXCR5+ HRS cells with ligand-expressing CXCL13+ macrophages as a prominent crosstalk axis in relapsed CHL. Harnessing this TME biology, we developed a novel prognostic model applicable to r/r CHL biopsies, RHL4S, opening new avenues for spatial biomarker development.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures

References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
