

Linking tumor immune infiltrate and systemic immune mediators to treatment response and prognosis in advanced cervical cancer
- PMID: 38114557
- PMCID: PMC10730812
- DOI: 10.1038/s41598-023-49441-2
Linking tumor immune infiltrate and systemic immune mediators to treatment response and prognosis in advanced cervical cancer
Abstract
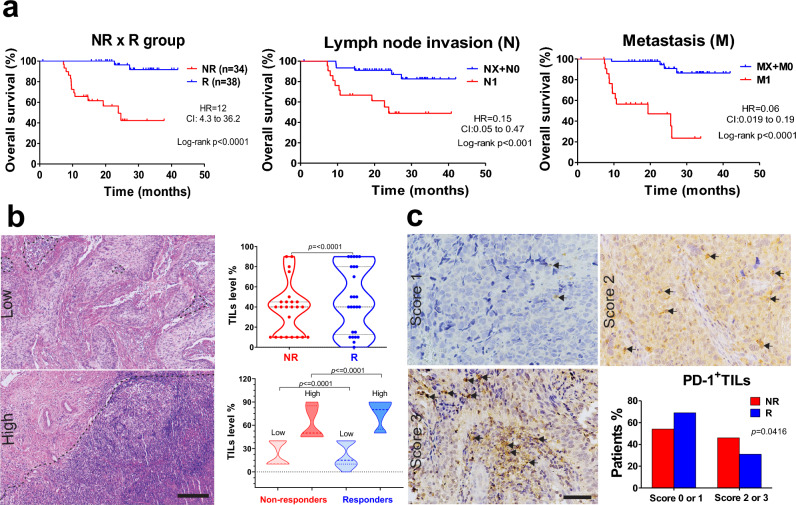
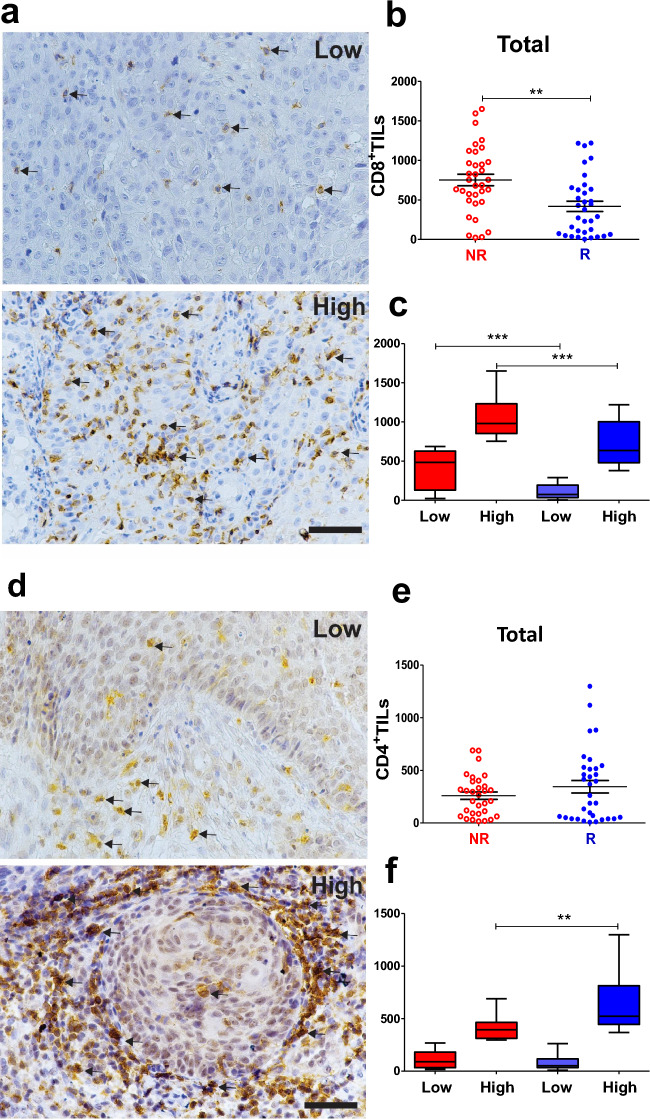
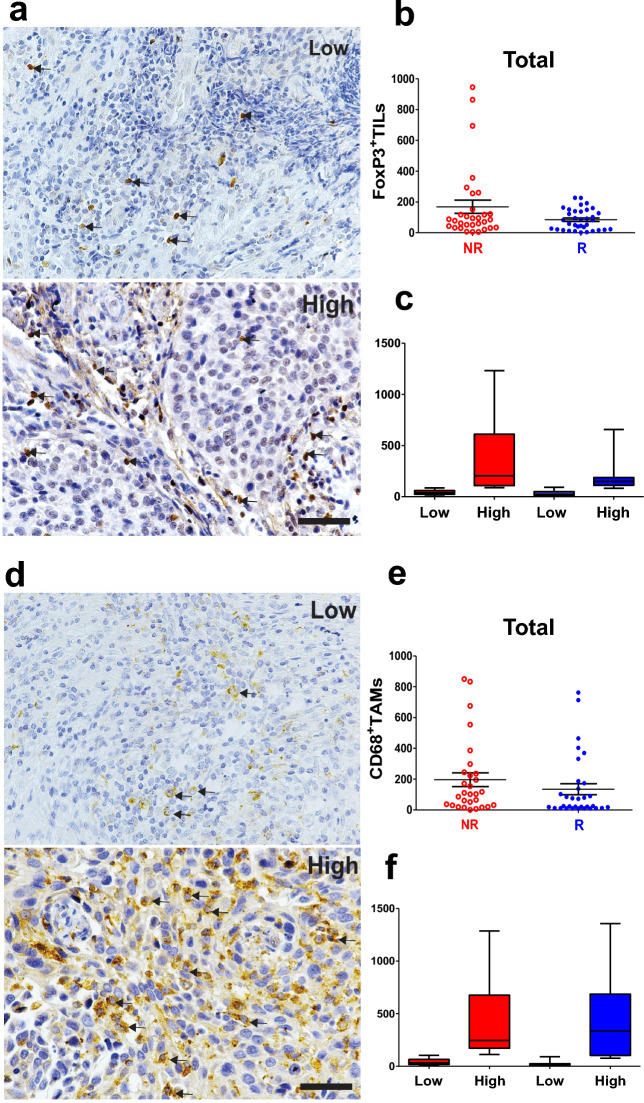
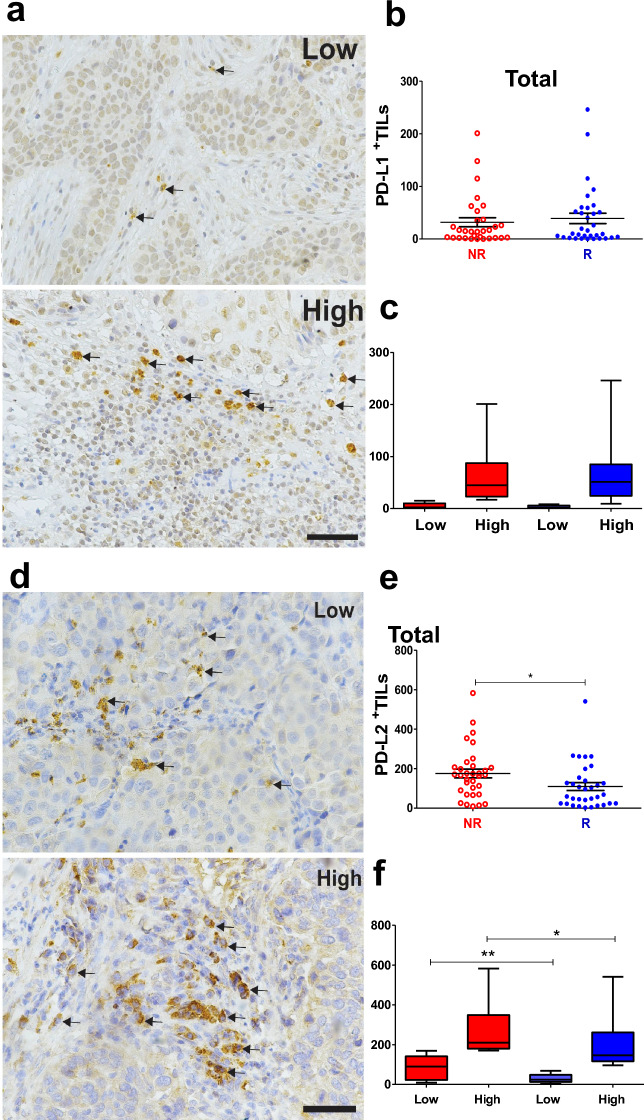
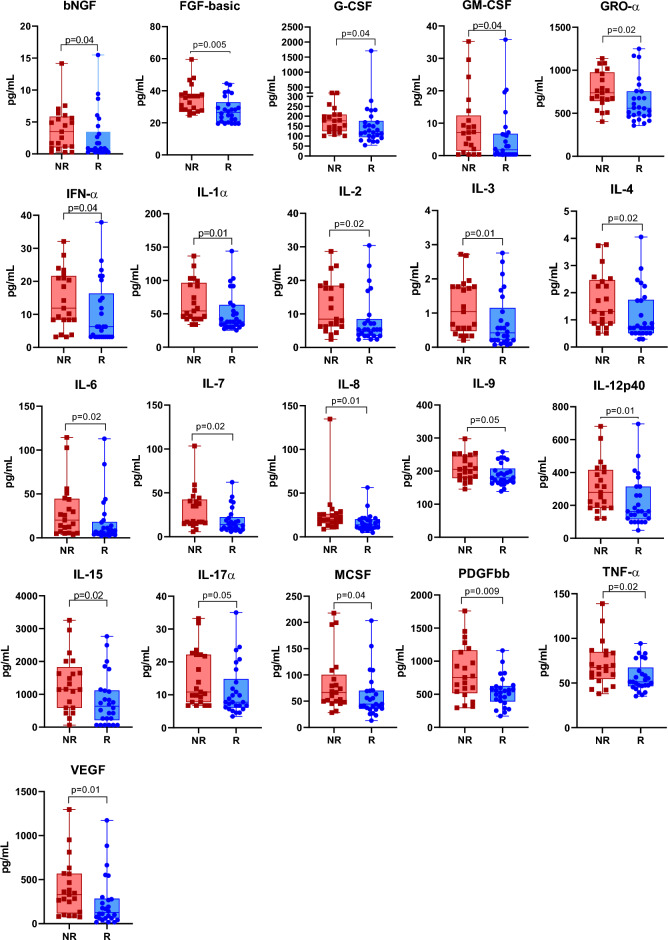
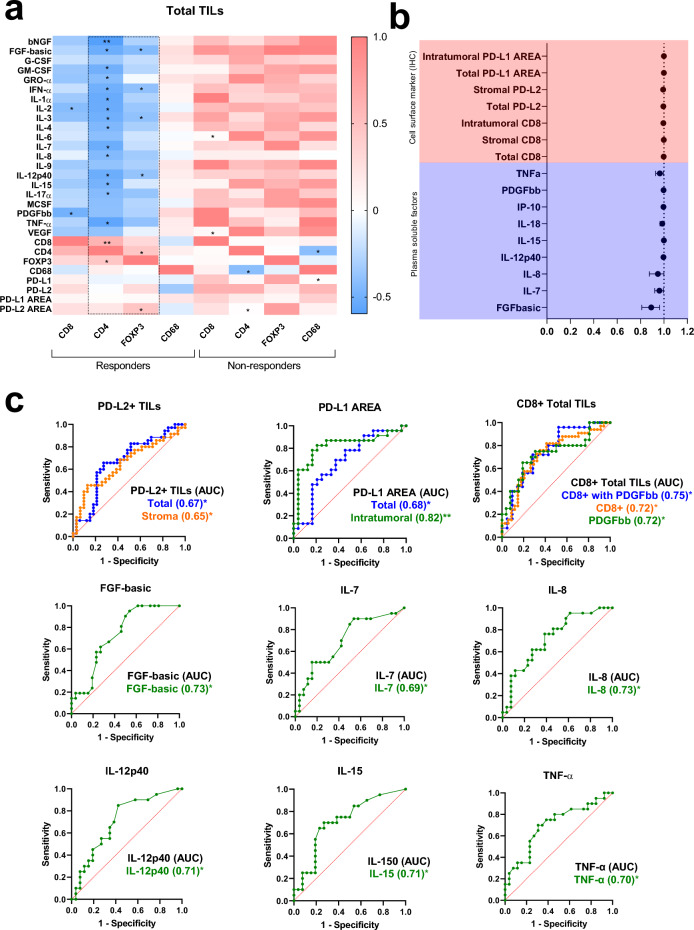
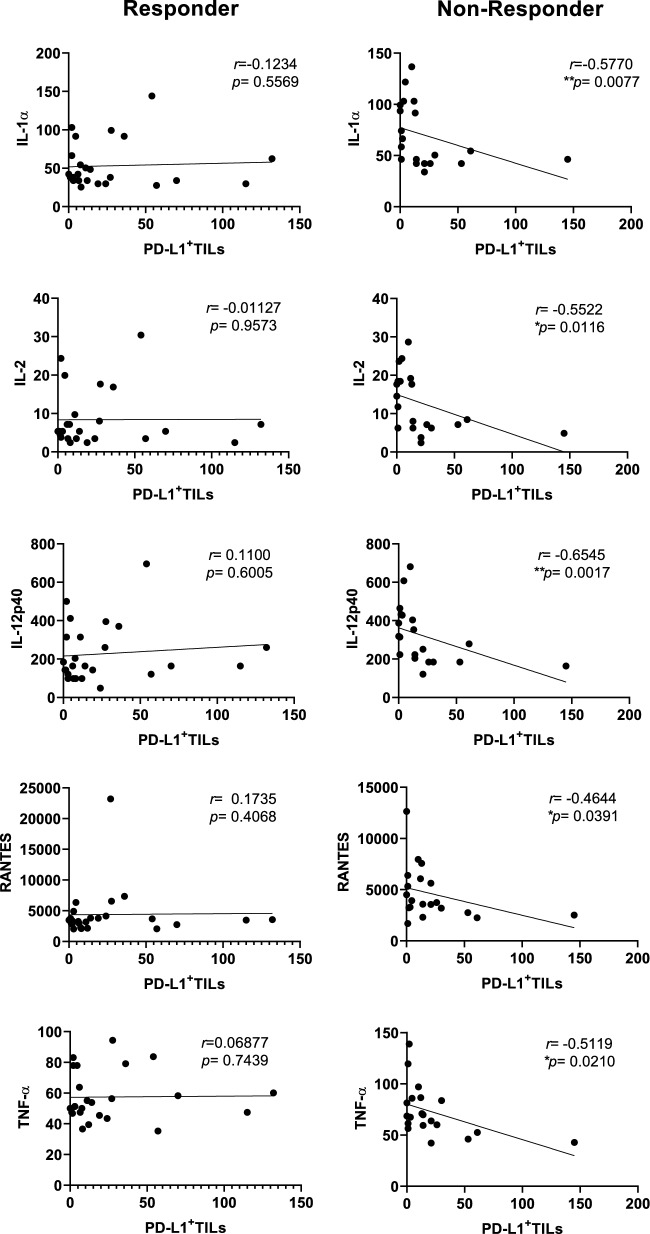
Cervical cancer (CC) poses a significant burden on individuals in developing regions, exhibiting heterogeneous responses to standard chemoradiation therapy, and contributing to substantial mortality rates. Unraveling host immune dynamics holds promise for innovative therapies and discovery of clinically relevant biomarkers. We studied prospectively locally advanced CC patients pre-treatment, stratifying them as responders (R) or non-responders (NR). R patients had increased tumor-infiltrating lymphocytes (TILs), while NR patients showed elevated PD-1 scores, CD8+ and PD-L2+ TILs, and PD-L1 immune reactivity. NR patients exhibited higher systemic soluble mediators correlating with TIL immune markers. R patients demonstrated functional polarization of CD4 T cells (Th1, Th2, Th17, and Treg), while CD8+ T cells and CD68+ macrophages predominated in the NR group. Receiver operating characteristic analysis identified potential CC response predictors, including PD-L1-immunoreactive (IR) area, PD-L2, CD8, FGF-basic, IL-7, IL-8, IL-12p40, IL-15, and TNF-alpha. Dysfunctional TILs and imbalanced immune mediators contribute to therapeutic insufficiency, shedding light on local and systemic immune interplay. Our study informs immunological signatures for treatment prediction and CC prognosis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
