

Inferior vena cava collapsibility index as a predictor of hypotension after induction of general anesthesia in hypertensive patients
- PMID: 38114949
- PMCID: PMC10729554
- DOI: 10.1186/s12871-023-02355-y
Inferior vena cava collapsibility index as a predictor of hypotension after induction of general anesthesia in hypertensive patients
Abstract
Background: Hypertensive patients are more susceptible to develop hypotension after the induction of general anesthesia (GA), most likely due to hypovolemia. An inferior vena cava collapsibility index (IVCCI) > 40-50% can predict hypotension after the induction of GA in the general population by variable accuracies. The current study aimed to investigate IVCCI% as a predictor of postinduction hypotension in hypertensive patients undergoing noncardiac surgery.
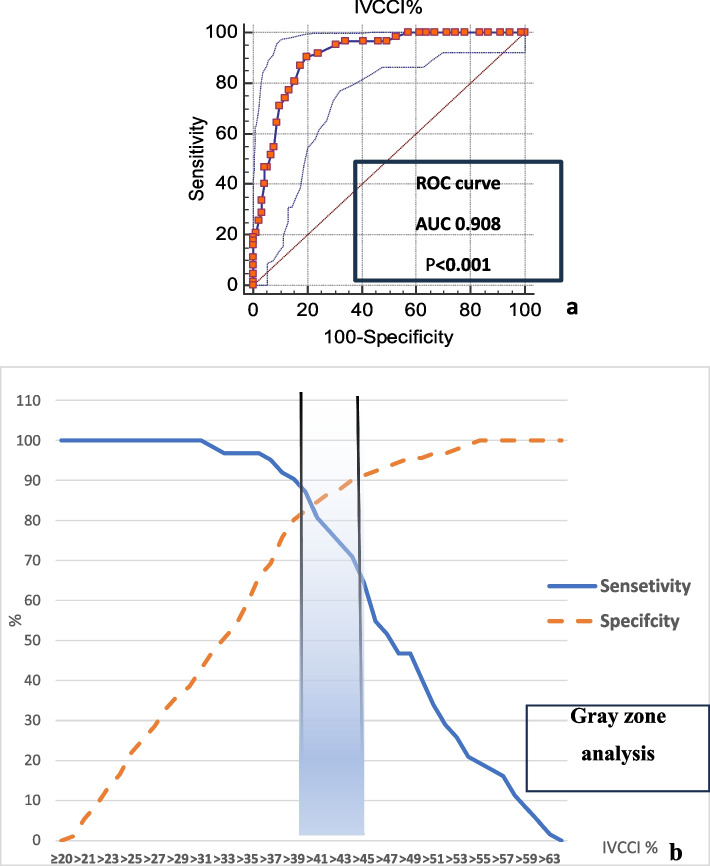
Methods: Ultrasound IVCCI % was assessed for all controlled hypertensive patients immediately before induction of GA. After induction of GA, patients were diagnosed with postinduction hypotension if their systolic arterial pressure (SAP) dropped by ≥ 30% of the baseline value and/or mean arterial pressure (MAP) dropped to < 65 mmHg up to 15 min after intubation. The receiver operating characteristic (ROC) curve of IVCCI% was compared to patients' classification either developing hypotension after induction of GA or not as a gold standard.
Results: Of the 153 patients who completed the study, 62 (40.5%) developed hypotension after the induction of GA, and 91 (59.5%) did not. An IVCCI > 39% predicted the occurrence of postinduction hypotension with high accuracy (84%) (AUC 0.908, P < 0.001). The area of uncertainty (by gray zone analysis) of IVCCI lies at values from 39 to 45%. This gray zone included 21 patients (13.7% of all patients).
Conclusion: An inferior vena cava collapsibility index > 39% before anesthetic induction can be a simple noninvasive reliable predictor of hypotension after the induction of GA for hypertensive patients not treated with angiotensin-converting enzyme inhibitors (ACEIs) or angiotensin receptor blockers (ARBs) and undergoing noncardiac surgery.
Trial registration: This clinical trial was approved by the Institutional Review Board (IRB) at Zagazig University (ZUIRB #9424 dated 03/04/2022), and patients' informed consent for participation in the study was obtained during the period from May 2022 to May 2023. All study procedures were carried out in accordance with the ethical standards of the Helsinki Declaration of 2013.
Keywords: Collapsibility index; General anesthesia; Hypertension; Hypotension; Inferior vena cava.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Bijker JB, van Klei WA, Kappen TH, van Wolfswinkel L, Moons KG, Kalkman CJ. Incidence of intraoperative hypotension as a function of the chosen definition: literature definitions applied to a retrospective cohort using automated data collection. J Am Soc Anesthesiologists. 2007;107(2):213–220. - PubMed
-
- Walsh M, Devereaux PJ, Garg AX, Kurz A, Turan A, Rodseth RN, et al. Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: toward an empirical definition of hypotension. Anesthesiology. 2013;119:507–515. doi: 10.1097/ALN.0b013e3182a10e26. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
