

Radiomics from multisite MRI and clinical data to predict clinically significant prostate cancer
- PMID: 38115809
- PMCID: PMC10964389
- DOI: 10.1177/02841851231216555
Radiomics from multisite MRI and clinical data to predict clinically significant prostate cancer
Abstract
Background: Magnetic resonance imaging (MRI) is useful in the diagnosis of clinically significant prostate cancer (csPCa). MRI-derived radiomics may support the diagnosis of csPCa.
Purpose: To investigate whether adding radiomics from biparametric MRI to predictive models based on clinical and MRI parameters improves the prediction of csPCa in a multisite-multivendor setting.
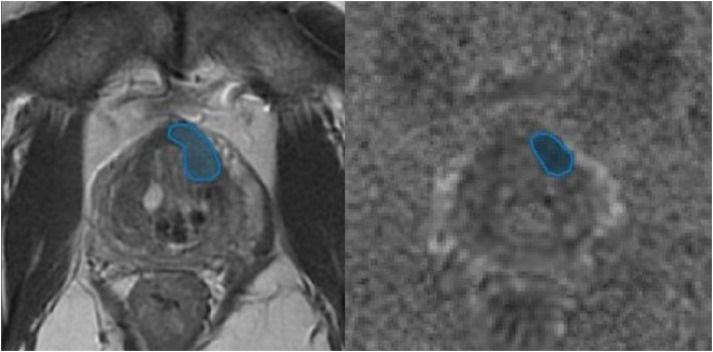
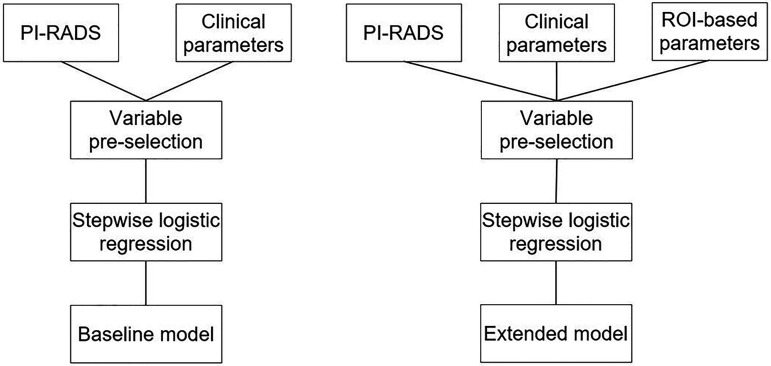
Material and methods: Clinical information (PSA, PSA density, prostate volume, and age), MRI reviews (PI-RADS 2.1), and radiomics (histogram and texture features) were retrieved from prospectively included patients examined at different radiology departments and with different MRI systems, followed by MRI-ultrasound fusion guided biopsies of lesions PI-RADS 3-5. Predictive logistic regression models of csPCa (Gleason score ≥7) for the peripheral (PZ) and transition zone (TZ), including clinical data and PI-RADS only, and combined with radiomics, were built and compared using receiver operating characteristic (ROC) curves.
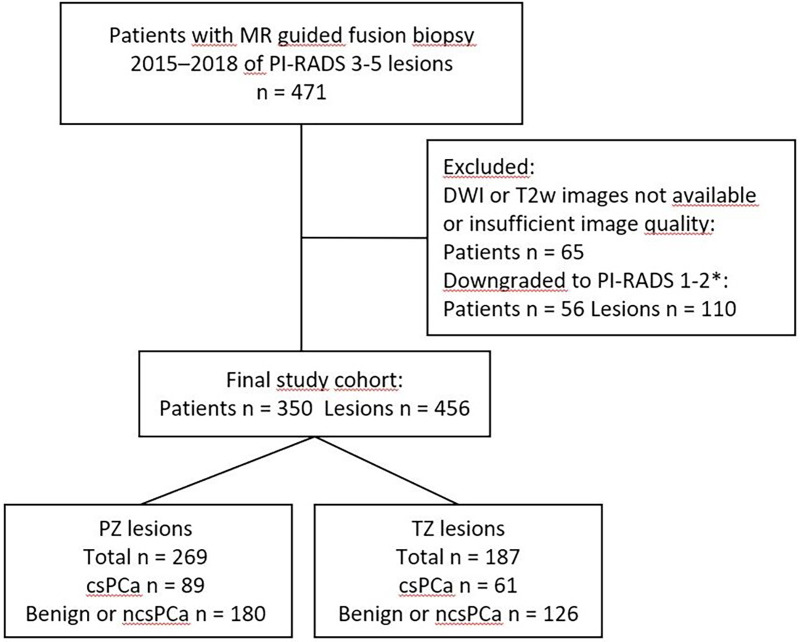
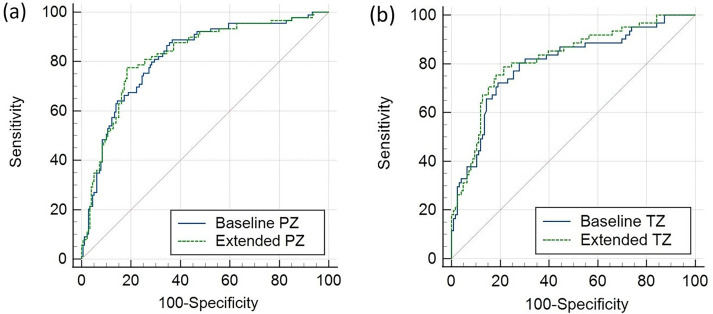
Results: In total, 456 lesions in 350 patients were analyzed. In PZ and TZ, PI-RADS 4-5 and PSA density, and age in PZ, were independent predictors of csPCa in models without radiomics. In models including radiomics, PI-RADS 4-5, PSA density, age, and ADC energy were independent predictors in PZ, and PI-RADS 5, PSA density and ADC mean in TZ. Comparison of areas under the ROC curve (AUC) for the models without radiomics (PZ: AUC = 0.82, TZ: AUC = 0.80) versus with radiomics (PZ: AUC = 0.82, TZ: AUC = 0.82) showed no significant differences (PZ: P = 0.366; TZ: P = 0.171).
Conclusion: PSA density and PI-RADS are potent predictors of csPCa. Radiomics do not add significant information to our multisite-multivendor dataset.
Keywords: PI-RADS; magnetic resonance imaging; multisite-multivendor; prostate cancer; radiomics.
Conflict of interest statement
Declaration of conflicting interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Roobol MJ, Steyerberg EW, Kranse R, et al. A risk-based strategy improves prostate-specific antigen-driven detection of prostate cancer. Eur Urol 2010;57:79–85. - PubMed
-
- Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate imaging reporting and data system version 2.1: 2019 update of Prostate Imaging Reporting and Data System version 2. Eur Urol 2019;76:340–351. - PubMed
-
- Alberts AR, Roobol MJ, Verbeek JFM, et al. Prediction of high-grade prostate cancer following multiparametric magnetic resonance imaging: improving the Rotterdam European Randomized Study of Screening for Prostate Cancer risk calculators. Eur Urol 2019;75:310–318. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
