

Laparoscopic anatomical versus non-anatomical liver resection for hepatocellular carcinoma in the posterosuperior segments: a propensity score matched analysis
- PMID: 38115923
- PMCID: PMC10727829
- DOI: 10.21037/hbsn-21-578
Laparoscopic anatomical versus non-anatomical liver resection for hepatocellular carcinoma in the posterosuperior segments: a propensity score matched analysis
Abstract
Background: Since laparoscopic anatomical resection (LAR) for tumors, especially located in the posterosuperior (PS) segments of the liver remains difficult, laparoscopic non-anatomical resection (LNAR) are generally preferred. To compare the clinical outcomes between LAR and LNAR for hepatocellular carcinoma (HCC) located in the PS segments.
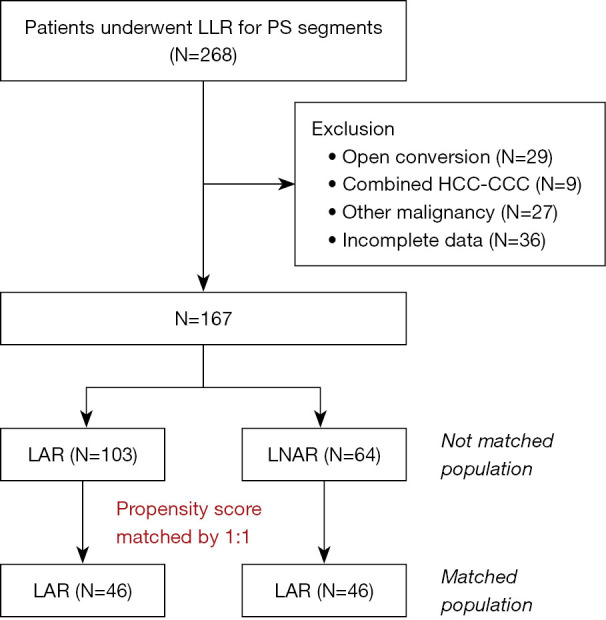
Methods: We retrospectively reviewed the data for 1,029 patients who underwent hepatectomy for HCC between 2004 and 2019. Of 167 patients who underwent laparoscopic hepatectomy for HCC in PS segments, 64 underwent LNAR and 103 underwent LAR. Patients were matched one-to-one using propensity score matching (46:46).
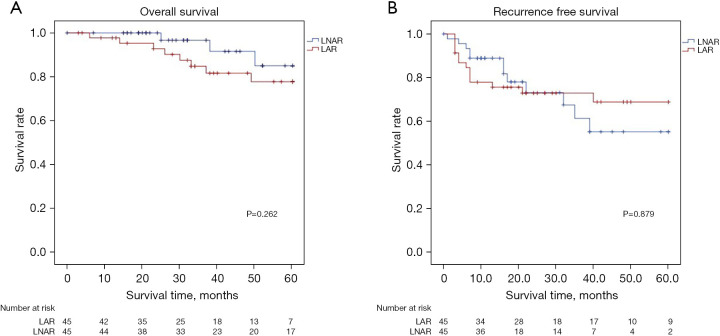
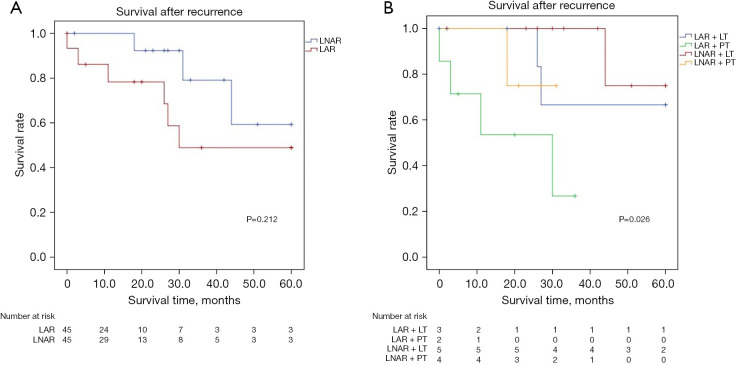
Results: LNAR was associated with significantly shorter operation time (P=0.001), lower estimated blood loss (P=0.001), lower transfusion rate (P=0.006) and shorter hospital stay (P=0.012) than LAR. The respective 1- ,3-, and 5-year overall survival rates (LAR: 95.3%, 87.1%, and 77.8%; LNAR: 96.7%, 91.6%, and 85.0%; P=0.262) and recurrence-free survival rates (LAR: 75.7%, 70.3%, and 68.9%; LNAR: 81.8%, 58.3%, and 55.3%; P=0.879) were similar. The intrahepatic recurrence rate was significantly higher in LNAR group than in LAR group (78.6% vs. 57.1%, P=0.023), but the post-recurrence treatments differed significantly between the two groups (P=0.016); the re-resection rate was much greater in the LNAR group (45.0% vs. 0%) group. The respective 1-, 3-, and 5-year post-recurrence survival rates were similar in the LAR and LNAR groups (P=0.212). After recurrence, survival in re-resection group was significantly greater than not (P=0.026).
Conclusions: LNAR is safe and feasible for HCC located in PS segments, and provided acceptable oncologic outcomes that are comparable to those of LAR. LNAR can be considered for patient with tumor located in PS segment when LAR is not feasible.
Keywords: Laparoscopy; carcinoma, hepatocellular; hepatectomy; recurrence.
2023 Hepatobiliary Surgery and Nutrition. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://hbsn.amegroups.com/article/view/10.21037/hbsn-21-578/coif). H.S.H. serves as an unpaid editorial board member of Hepatobiliary Surgery and Nutrition. J.Y.C. receives support (Grant No. 02-2021-046) from Seoul National University Bundang Hospital Research Fund. The other authors have no conflicts of interest to declare.
Figures
Comment in
-
Anatomical or non-anatomical resections for hepatocellular carcinoma: a never-ending debate.Hepatobiliary Surg Nutr. 2025 Apr 1;14(2):342-344. doi: 10.21037/hbsn-2025-49. Epub 2025 Mar 25. Hepatobiliary Surg Nutr. 2025. PMID: 40342773 Free PMC article. No abstract available.
References
-
- Makuuchi M, Hasegawa H, Yamazaki S. Ultrasonically guided subsegmentectomy. Surg Gynecol Obstet 1985;161:346-50. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous