

Consumption of ultra-processed foods and risk of multimorbidity of cancer and cardiometabolic diseases: a multinational cohort study
- PMID: 38115963
- PMCID: PMC10730313
- DOI: 10.1016/j.lanepe.2023.100771
Consumption of ultra-processed foods and risk of multimorbidity of cancer and cardiometabolic diseases: a multinational cohort study
Abstract
Background: It is currently unknown whether ultra-processed foods (UPFs) consumption is associated with a higher incidence of multimorbidity. We examined the relationship of total and subgroup consumption of UPFs with the risk of multimorbidity defined as the co-occurrence of at least two chronic diseases in an individual among first cancer at any site, cardiovascular disease, and type 2 diabetes.
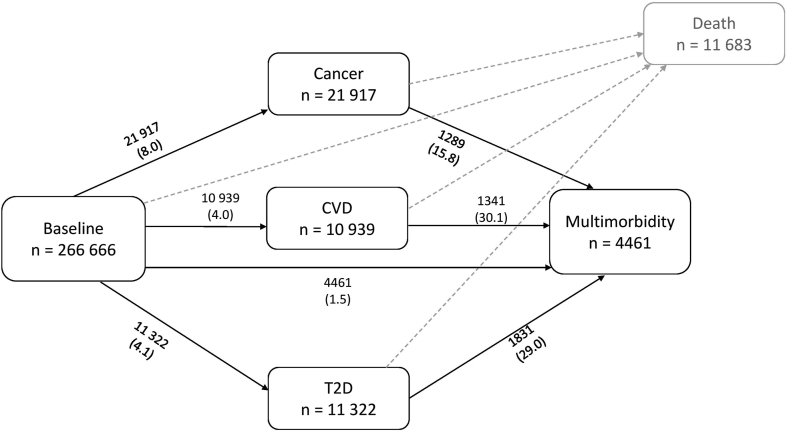
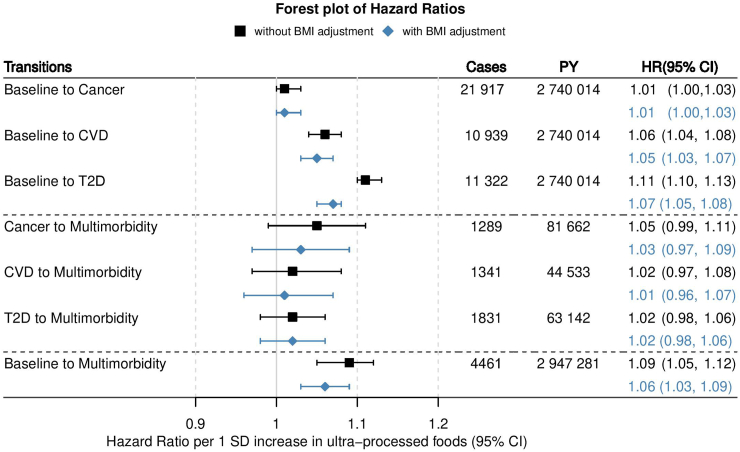
Methods: This was a prospective cohort study including 266,666 participants (60% women) free of cancer, cardiovascular disease, and type 2 diabetes at recruitment from seven European countries in the European Prospective Investigation into Cancer and Nutrition (EPIC) study. Foods and drinks consumed over the previous 12 months were assessed at baseline by food-frequency questionnaires and classified according to their degree of processing using Nova classification. We used multistate modelling based on Cox regression to estimate cause-specific hazard ratios (HR) and their 95% confidence intervals (CI) for associations of total and subgroups of UPFs with the risk of multimorbidity of cancer and cardiometabolic diseases.
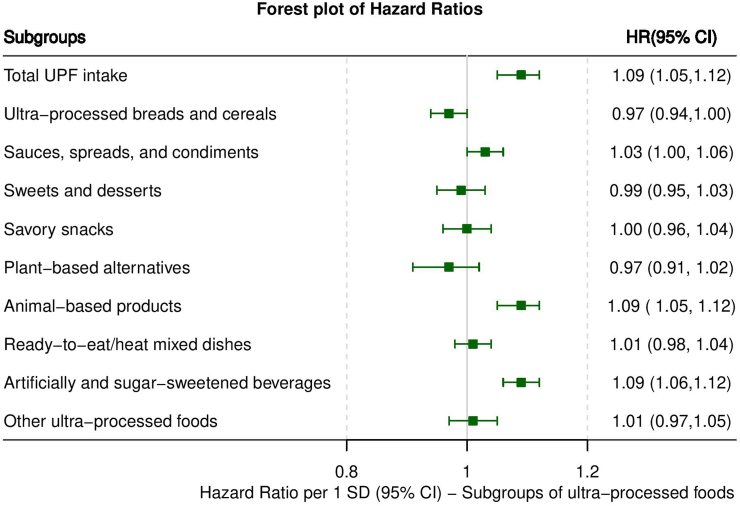
Findings: After a median of 11.2 years of follow-up, 4461 participants (39% women) developed multimorbidity of cancer and cardiometabolic diseases. Higher UPF consumption (per 1 standard deviation increment, ∼260 g/day without alcoholic drinks) was associated with an increased risk of multimorbidity of cancer and cardiometabolic diseases (HR: 1.09, 95% CI: 1.05, 1.12). Among UPF subgroups, associations were most notable for animal-based products (HR: 1.09, 95% CI: 1.05, 1.12), and artificially and sugar-sweetened beverages (HR: 1.09, 95% CI: 1.06, 1.12). Other subgroups such as ultra-processed breads and cereals (HR: 0.97, 95% CI: 0.94, 1.00) or plant-based alternatives (HR: 0.97, 95% CI: 0.91, 1.02) were not associated with risk.
Interpretation: Our findings suggest that higher consumption of UPFs increases the risk of cancer and cardiometabolic multimorbidity.
Funding: Austrian Academy of Sciences, Fondation de France, Cancer Research UK, World Cancer Research Fund International, and the Institut National du Cancer.
Keywords: Cancer; Cardiovascular diseases; Diabetes; Diet; Multimorbidity; Ultra-processed foods.
© 2023 Published by Elsevier Ltd.
Conflict of interest statement
None of the authors declared a competing interest.
Figures
References
-
- Mendis S. World Health Organization; Geneva, Switzerland: 2014. Global status report on noncommunicable diseases 2014. - PubMed
-
- Academy of Medical Sciences (Royaume uni) Academy of Medical Sciences; 2018. Multimorbidity: a priority for global health research.
Grants and funding
LinkOut - more resources
Full Text Sources
