

Pendelluft in hypoxemic patients resuming spontaneous breathing: proportional modes versus pressure support ventilation
- PMID: 38117367
- PMCID: PMC10733241
- DOI: 10.1186/s13613-023-01230-w
Pendelluft in hypoxemic patients resuming spontaneous breathing: proportional modes versus pressure support ventilation
Abstract
Background: Internal redistribution of gas, referred to as pendelluft, is a new potential mechanism of effort-dependent lung injury. Neurally-adjusted ventilatory assist (NAVA) and proportional assist ventilation (PAV +) follow the patient's respiratory effort and improve synchrony compared with pressure support ventilation (PSV). Whether these modes could prevent the development of pendelluft compared with PSV is unknown. We aimed to compare pendelluft magnitude during PAV + and NAVA versus PSV in patients with resolving acute respiratory distress syndrome (ARDS).
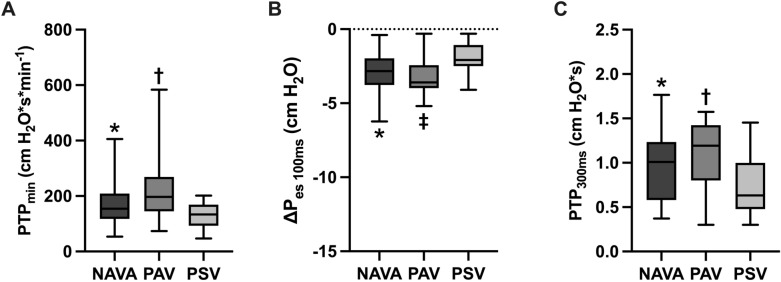
Methods: Patients received either NAVA, PAV + , or PSV in a crossover trial for 20-min using comparable assistance levels after controlled ventilation (> 72 h). We assessed pendelluft (the percentage of lost volume from the non-dependent lung region displaced to the dependent region during inspiration), drive (as the delta esophageal swing of the first 100 ms [ΔPes 100 ms]) and inspiratory effort (as the esophageal pressure-time product per minute [PTPmin]). We performed repeated measures analysis with post-hoc tests and mixed-effects models.
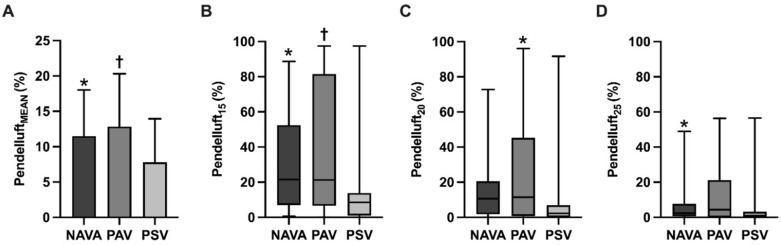
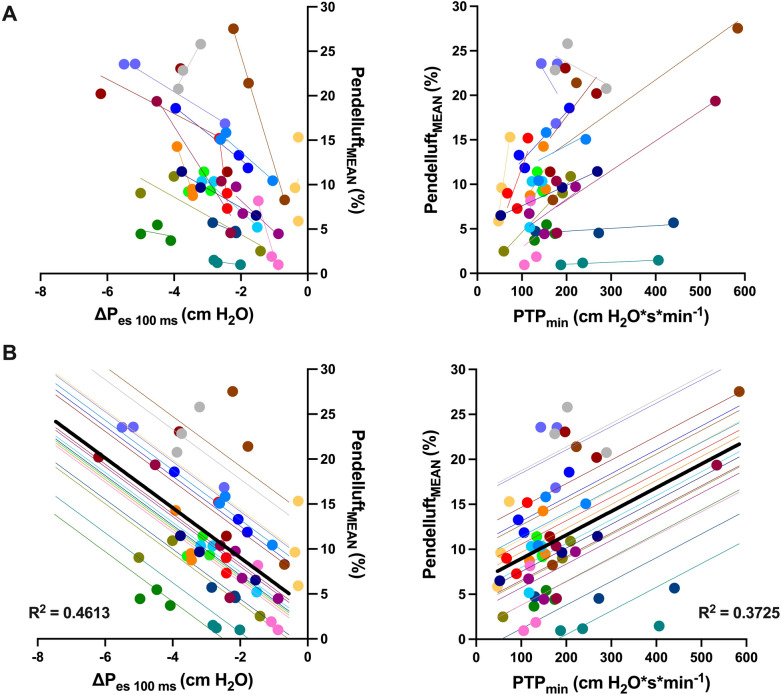
Results: Twenty patients mechanically ventilated for 9 [5-14] days were monitored. Despite matching for a similar tidal volume, respiratory drive and inspiratory effort were slightly higher with NAVA and PAV + compared with PSV (ΔPes 100 ms of -2.8 [-3.8--1.9] cm H2O, -3.6 [-3.9--2.4] cm H2O and -2.1 [-2.5--1.1] cm H2O, respectively, p < 0.001 for both comparisons; PTPmin of 155 [118-209] cm H2O s/min, 197 [145-269] cm H2O s/min, and 134 [93-169] cm H2O s/min, respectively, p < 0.001 for both comparisons). Pendelluft magnitude was higher in NAVA (12 ± 7%) and PAV + (13 ± 7%) compared with PSV (8 ± 6%), p < 0.001. Pendelluft magnitude was strongly associated with respiratory drive (β = -2.771, p-value < 0.001) and inspiratory effort (β = 0.026, p < 0.001), independent of the ventilatory mode. A higher magnitude of pendelluft in proportional modes compared with PSV existed after adjusting for PTPmin (β = 2.606, p = 0.010 for NAVA, and β = 3.360, p = 0.004 for PAV +), and only for PAV + when adjusted for respiratory drive (β = 2.643, p = 0.009 for PAV +).
Conclusions: Pendelluft magnitude is associated with respiratory drive and inspiratory effort. Proportional modes do not prevent its occurrence in resolving ARDS compared with PSV.
Keywords: Acute respiratory distress syndrome; Neurally-adjusted ventilatory assist; Pendelluft; Pressure support ventilation; Proportional assist ventilation.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
