

Dual Antiplatelet Therapy De-Escalation in Stabilized Myocardial Infarction With High Ischemic Risk: Post Hoc Analysis of the TALOS-AMI Randomized Clinical Trial
- PMID: 38117483
- PMCID: PMC10733848
- DOI: 10.1001/jamacardio.2023.4587
Dual Antiplatelet Therapy De-Escalation in Stabilized Myocardial Infarction With High Ischemic Risk: Post Hoc Analysis of the TALOS-AMI Randomized Clinical Trial
Abstract
Importance: In patients with acute myocardial infarction (AMI) who have high ischemic risk, data on the efficacy and safety of the de-escalation strategy of switching from ticagrelor to clopidogrel are lacking.
Objective: To evaluate the outcomes of the de-escalation strategy compared with dual antiplatelet therapy (DAPT) with ticagrelor in stabilized patients with AMI and high ischemic risk following percutaneous coronary intervention (PCI).
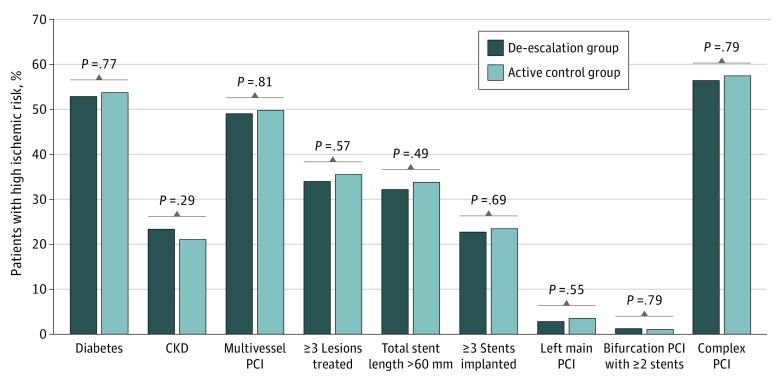
Design, setting, and participants: This was a post hoc analysis of the Ticagrelor vs Clopidogrel in Stabilized Patients With Acute Myocardial Infarction (TALOS-AMI) trial, an open-label, assessor-blinded, multicenter, randomized clinical trial. Patients with AMI who had no event during 1 month of ticagrelor-based DAPT after PCI were included. High ischemic risk was defined as having a history of diabetes or chronic kidney disease, multivessel PCI, at least 3 lesions treated, total stent length greater than 60 mm, at least 3 stents implanted, left main PCI, or bifurcation PCI with at least 2 stents. Data were collected from February 14, 2014, to January 21, 2021, and analyzed from December 1, 2021, to June 30, 2022.
Intervention: Patients were randomly assigned to either de-escalation from ticagrelor to clopidogrel or ticagrelor-based DAPT.
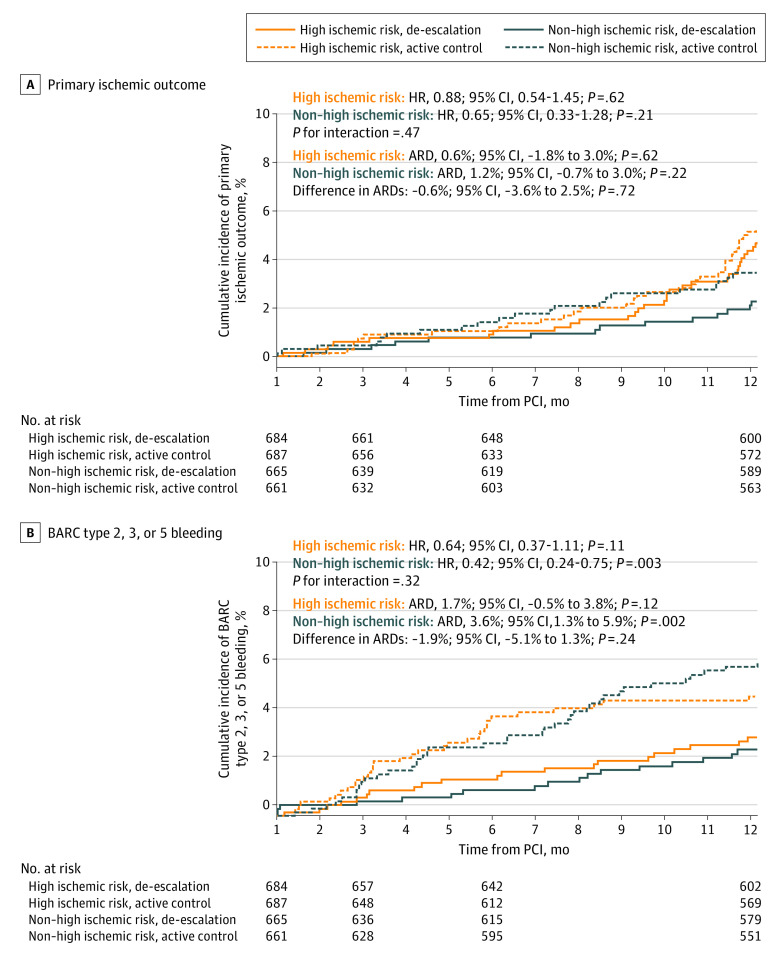
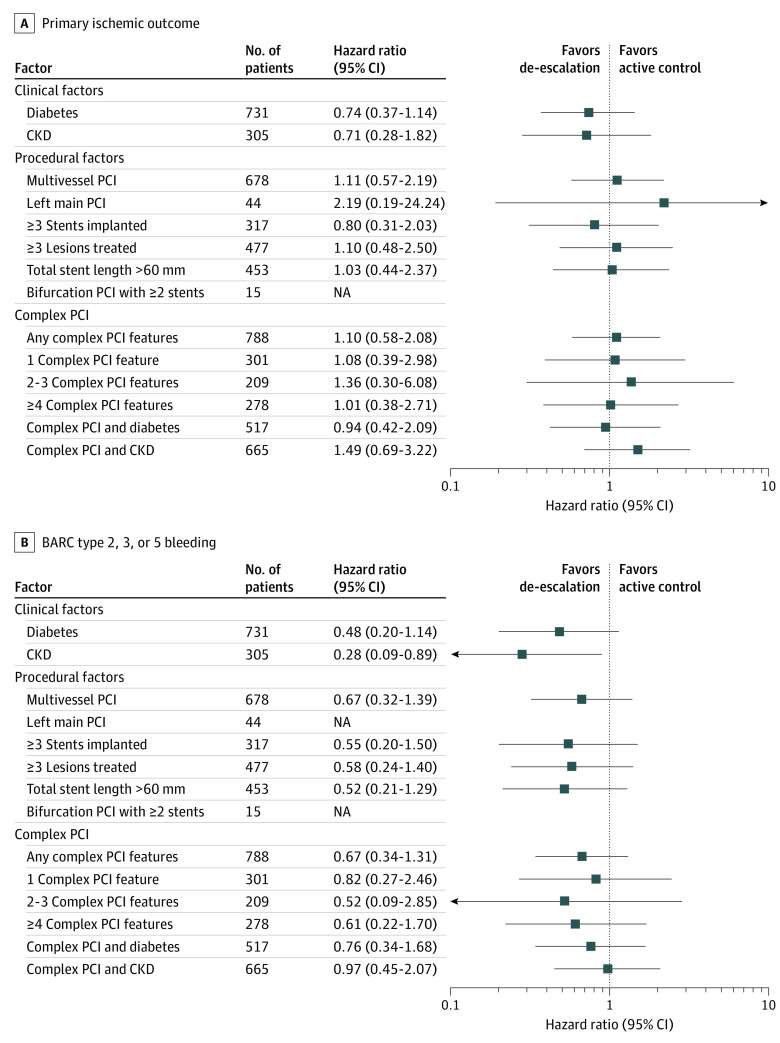
Main outcomes and measures: Ischemic outcomes (composite of cardiovascular death, myocardial infarction, ischemic stroke, ischemia-driven revascularization, or stent thrombosis) and bleeding outcomes (Bleeding Academic Research Consortium type 2, 3, or 5 bleeding) were evaluated.
Results: Of 2697 patients with AMI (mean [SD] age, 60.0 [11.4] years; 454 [16.8%] female), 1371 (50.8%; 684 assigned to de-escalation and 687 assigned to ticagrelor-based DAPT) had high ischemic risk features and a significantly higher risk of ischemic outcomes than those without high ischemic risk (1326 patients [49.2%], including 665 assigned to de-escalation and 661 assigned to ticagrelor-based DAPT) (hazard ratio [HR], 1.74; 95% CI, 1.15-2.63; P = .01). De-escalation to clopidogrel, compared with ticagrelor-based DAPT, showed no significant difference in ischemic risk across the high ischemic risk group (HR, 0.88; 95% CI, 0.54-1.45; P = .62) and the non-high ischemic risk group (HR, 0.65; 95% CI, 0.33-1.28; P = .21), without heterogeneity (P for interaction = .47). The bleeding risk of the de-escalation group was consistent in both the high ischemic risk group (HR, 0.64; 95% CI, 0.37-1.11; P = .11) and the non-high ischemic risk group (HR, 0.42; 95% CI, 0.24-0.75; P = .003), without heterogeneity (P for interaction = .32).
Conclusions and relevance: In stabilized patients with AMI, the ischemic and bleeding outcomes of an unguided de-escalation strategy with clopidogrel compared with a ticagrelor-based DAPT strategy were consistent without significant interaction, regardless of the presence of high ischemic risk.
Conflict of interest statement
Figures
References
-
- Lawton JS, Tamis-Holland JE, Bangalore S, et al. ; Writing Committee Members . 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(2):e21-e129. doi:10.1016/j.jacc.2021.09.006 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
