

Preoperative Midazolam and Patient-Centered Outcomes of Older Patients: The I-PROMOTE Randomized Clinical Trial
- PMID: 38117527
- PMCID: PMC10733850
- DOI: 10.1001/jamasurg.2023.6479
Preoperative Midazolam and Patient-Centered Outcomes of Older Patients: The I-PROMOTE Randomized Clinical Trial
Abstract
Importance: The effect of oral midazolam premedication on patient satisfaction in older patients undergoing surgery is unclear, despite its widespread use.
Objective: To determine the differences in global perioperative satisfaction in patients with preoperative administration of oral midazolam compared with placebo.
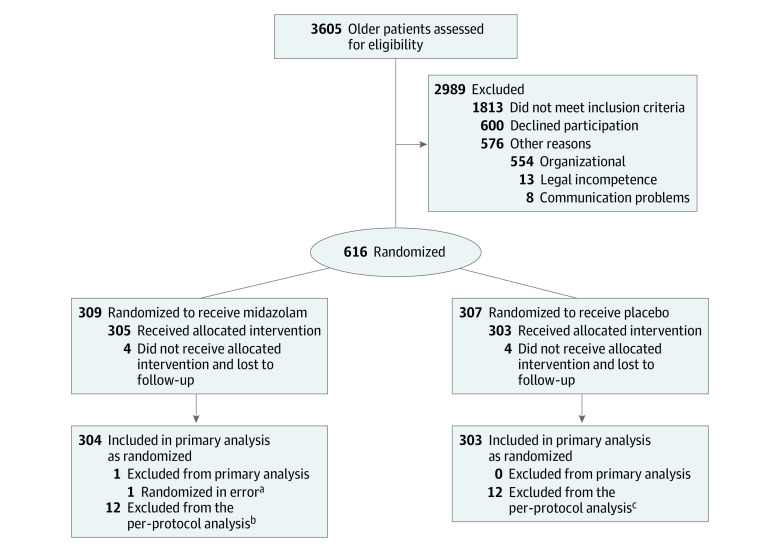
Design, setting, and participants: This double-blind, parallel-group, placebo-controlled randomized clinical trial was conducted in 9 German hospitals between October 2017 and May 2019 (last follow-up, June 24, 2019). Eligible patients aged 65 to 80 years who were scheduled for elective inpatient surgery for at least 30 minutes under general anesthesia and with planned extubation were enrolled. Data were analyzed from November 2019 to December 2020.
Interventions: Patients were randomized to receive oral midazolam, 3.75 mg (n = 309), or placebo (n = 307) 30 to 45 minutes prior to anesthesia induction.
Main outcomes and measures: The primary outcome was global patient satisfaction evaluated using the self-reported Evaluation du Vécu de l'Anesthésie Generale (EVAN-G) questionnaire on the first postoperative day. Key secondary outcomes included sensitivity and subgroup analyses of the primary outcome, perioperative patient vital data, adverse events, serious complications, and cognitive and functional recovery up to 30 days postoperatively.
Results: Among 616 randomized patients, 607 were included in the primary analysis. Of these, 377 (62.1%) were male, and the mean (SD) age was 71.9 (4.4) years. The mean (SD) global index of patient satisfaction did not differ between the midazolam and placebo groups (69.5 [10.7] vs 69.6 [10.8], respectively; mean difference, -0.2; 95% CI, -1.9 to 1.6; P = .85). Sensitivity (per-protocol population, multiple imputation) and subgroup analyses (anxiety, frailty, sex, and previous surgical experience) did not alter the primary results. Secondary outcomes did not differ, except for a higher proportion of patients with hypertension (systolic blood pressure ≥160 mm Hg) at anesthesia induction in the placebo group.
Conclusion and relevance: A single low dose of oral midazolam premedication did not alter the global perioperative patient satisfaction of older patients undergoing surgery or that of patients with anxiety. These results may be affected by the low dose of oral midazolam. Further trials-including a wider population with commonplace low-dose intravenous midazolam and plasma level measurements-are needed.
Trial registration: ClinicalTrials.gov Identifier: NCT03052660.
Conflict of interest statement
Figures
Comment in
-
Midazolam for Pregeneral Anesthesia Sedation-Aiming for Better Satisfaction in Elderly Patients.JAMA Surg. 2024 Feb 1;159(2):139. doi: 10.1001/jamasurg.2023.6493. JAMA Surg. 2024. PMID: 38117488 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
