

GIInger predicts homologous recombination deficiency and patient response to PARPi treatment from shallow genomic profiles
- PMID: 38118421
- PMCID: PMC10772634
- DOI: 10.1016/j.xcrm.2023.101344
GIInger predicts homologous recombination deficiency and patient response to PARPi treatment from shallow genomic profiles
Abstract
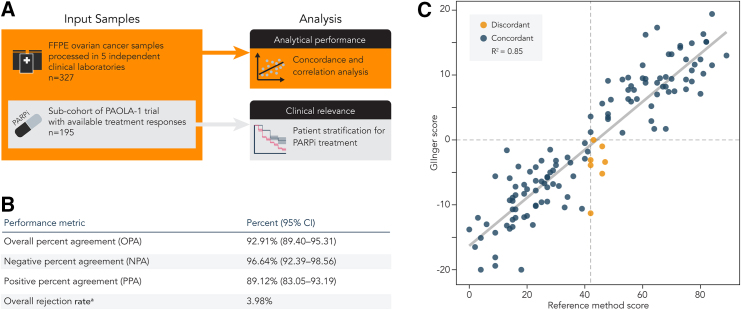
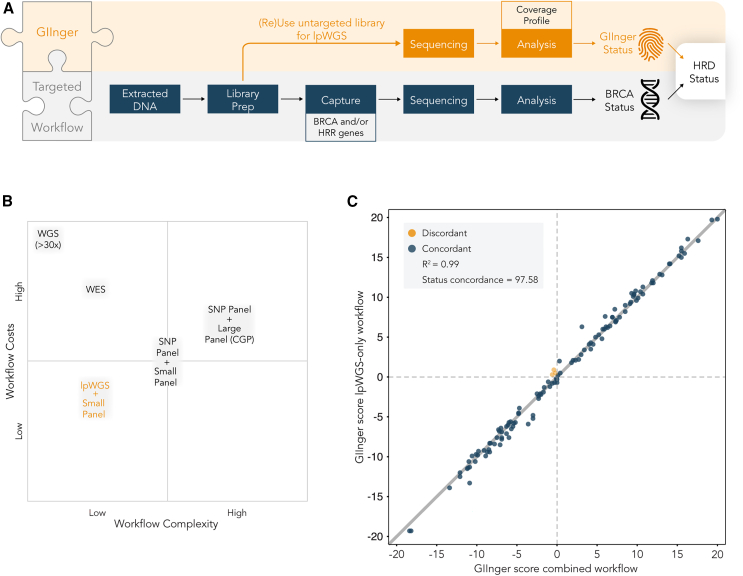
Homologous recombination deficiency (HRD) is a predictive biomarker for poly(ADP-ribose) polymerase 1 inhibitor (PARPi) sensitivity. Routine HRD testing relies on identifying BRCA mutations, but additional HRD-positive patients can be identified by measuring genomic instability (GI), a consequence of HRD. However, the cost and complexity of available solutions hamper GI testing. We introduce a deep learning framework, GIInger, that identifies GI from HRD-induced scarring observed in low-pass whole-genome sequencing data. GIInger seamlessly integrates into standard BRCA testing workflows and yields reproducible results concordant with a reference method in a multisite study of 327 ovarian cancer samples. Applied to a BRCA wild-type enriched subgroup of 195 PAOLA-1 clinical trial patients, GIInger identified HRD-positive patients who experienced significantly extended progression-free survival when treated with PARPi. GIInger is, therefore, a cost-effective and easy-to-implement method for accurately stratifying patients with ovarian cancer for first-line PARPi treatment.
Keywords: HRD; PARPi; biomarker; breast cancer; cancer; convolutional neural network; homologous recombination deficiency; low-pass whole-genome sequencing; lpWGS; ovarian cancer.
Copyright © 2023 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests G.A., T.C., C.P., J.B., R.K., L.F., A.S., F.C.B., L.R., A.A., R.M., M.F., A.C.M., E.S., A.W., and Z.X. are SOPHiA GENETICS employees. A.H. received consultant fees from SOPHiA GENETICS and honoraria from AstraZeneca, Janssen, and GSK. P.G. received honoraria from AstraZeneca. M.B. has received honoraria for consulting, advisory role, speakers’ bureau, travel, accommodation, and expenses from MSD Oncology, Roche/Genetech, AstraZeneca, Thermo Fisher Scientific, and Illumina. S.P. has received honoraria and research funding from AstraZeneca, MSD, GSK, and Roche and honoraria from Clovis. E.P.-L. served on a data safety monitoring board for Agenus Incyte, as a consultant for Roche, and as an advisory board member for AstraZeneca and GSK. I.V. as a consulting or advisory role at AstraZeneca. P.-A.J. has conducted teaching events for GSK, Roche, and EISAI. N.C. has reported fees for advisory board membership for AstraZeneca, Clovis Oncology, Eisai, GSK, Immunogen, Mersana, MSD/Merck, Nuvation Bio, Onxerna, Pfizer, Pieris, and Roche; fees as an invited speaker for AstraZeneca, Novartis, Clovis Oncology, GSK, and MSD/Merck; and institutional research grants from AstraZeneca and Roche. She has also reported non-remunerated activities as a member of the ESMO Guidelines Steering Committee and chair of the Scientific Committee of ACTO (Alleanza contro il tumore ovarico). A.G.-M. has received fees for different educational or advisory-related activities from Alkermes, AstraZeneca, Clovis, Genmab, GSK, HederaDx, Immunogen, Illumina, Mersana, MSD, Novartis, Novocure, Oncoinvent, PharmaMar, Roche, SOTIO, SUTRO, Seagen, and Takeda. P.H. has received honoraria from AstraZeneca, Roche, Sotio, Tesaro, Stryker, ASCO, Zai Lab, and MSD and has acted in advisory/consultancy for AstraZeneca, Roche, Tesaro, Lilly, Clovis, Immunogen, and MSD/Merck.
Figures




References
-
- Hanahan D., Weinberg R.A. Holland-Frei Cancer Medicine. John Wiley & Sons, Ltd; 2017. Biological Hallmarks of Cancer; pp. 1–10.
-
- O’Kane G.M., Connor A.A., Gallinger S. Characterization, Detection, and Treatment Approaches for Homologous Recombination Deficiency in Cancer. Trends Mol. Med. 2017;23:1121–1137. - PubMed
-
- Lord C.J., Ashworth A. BRCAness revisited. Nat. Rev. Cancer. 2016;16:110–120. - PubMed
-
- Moore K., Colombo N., Scambia G., Kim B.-G., Oaknin A., Friedlander M., Lisyanskaya A., Floquet A., Leary A., Sonke G.S., et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018;379:2495–2505. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
