

Marked irregular myofiber shape is a hallmark of human skeletal muscle ageing and is reversed by heavy resistance training
- PMID: 38123165
- PMCID: PMC10834339
- DOI: 10.1002/jcsm.13405
Marked irregular myofiber shape is a hallmark of human skeletal muscle ageing and is reversed by heavy resistance training
Abstract
Background: Age-related loss of strength is disproportionally greater than the loss of mass, suggesting maladaptations in the neuro-myo-tendinous system. Myofibers are often misshaped in aged and diseased muscle, but systematic analyses of large sample sets are lacking. Our aim was to investigate myofiber shape in relation to age, exercise, myofiber type, species and sex.
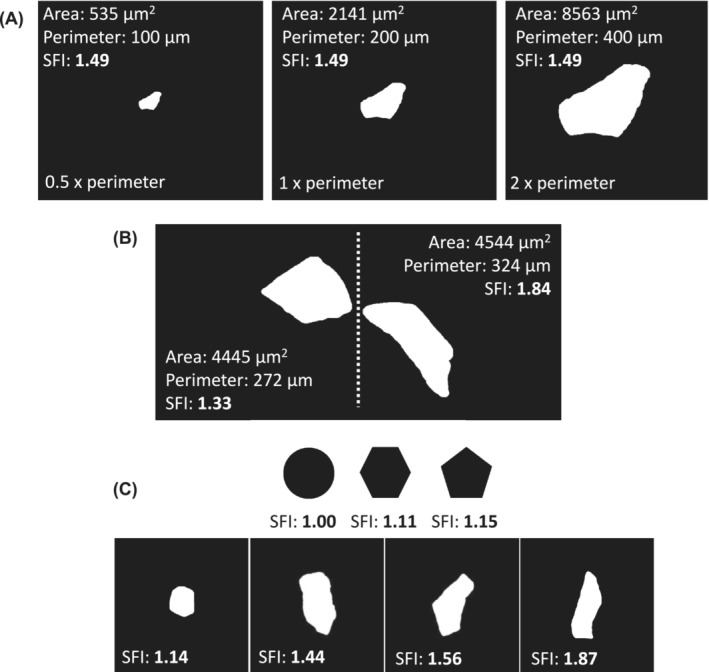
Methods: Vastus lateralis muscle biopsies (n = 265) from 197 males and females, covering an age span of 20-97 years, were examined. The gastrocnemius and soleus muscles of 11 + 22-month-old male C57BL/6 mice were also examined. Immunofluorescence and ATPase stainings of muscle cross-sections were used to measure myofiber cross-sectional area (CSA) and perimeter. From these, a shape factor index (SFI) was calculated in a fibre-type-specific manner (type I/II in humans; type I/IIa/IIx/IIb in mice), with higher values indicating increased deformity. Heavy resistance training (RT) was performed three times per week for 3-4 months by a subgroup (n = 59). Correlation analyses were performed comparing SFI and CSA with age, muscle mass, maximal voluntary contraction (MVC), rate of force development and specific force (MVC/muscle mass).
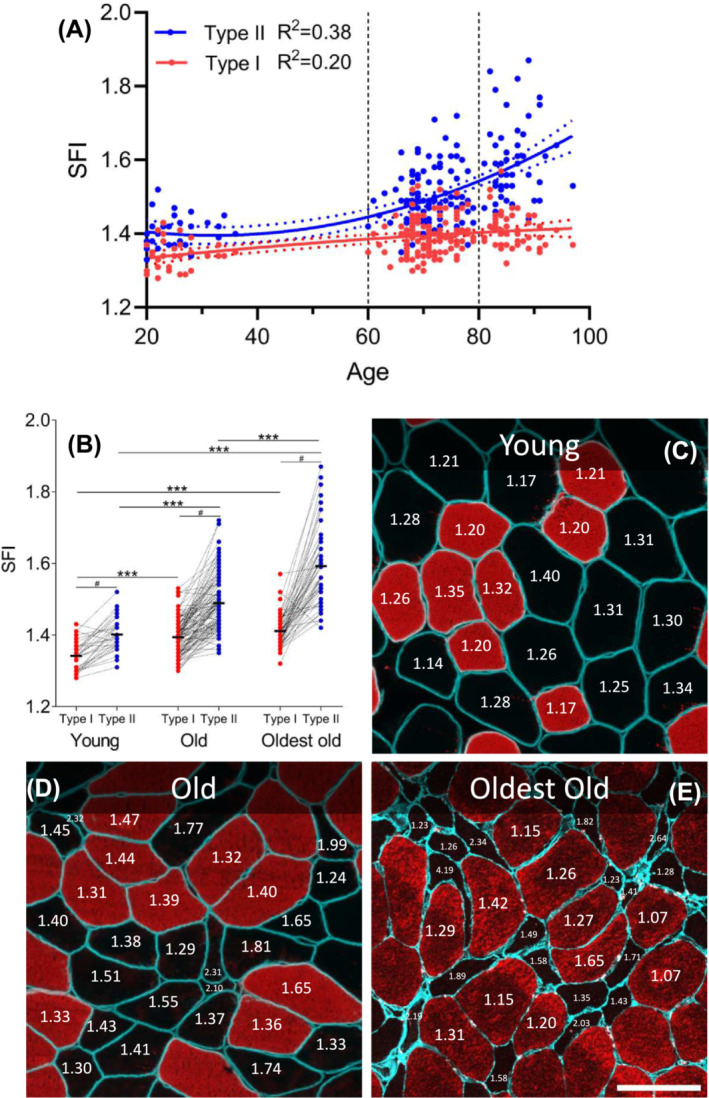
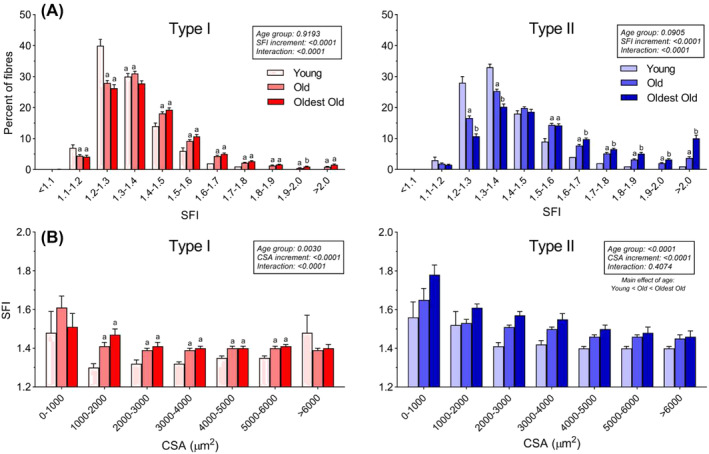
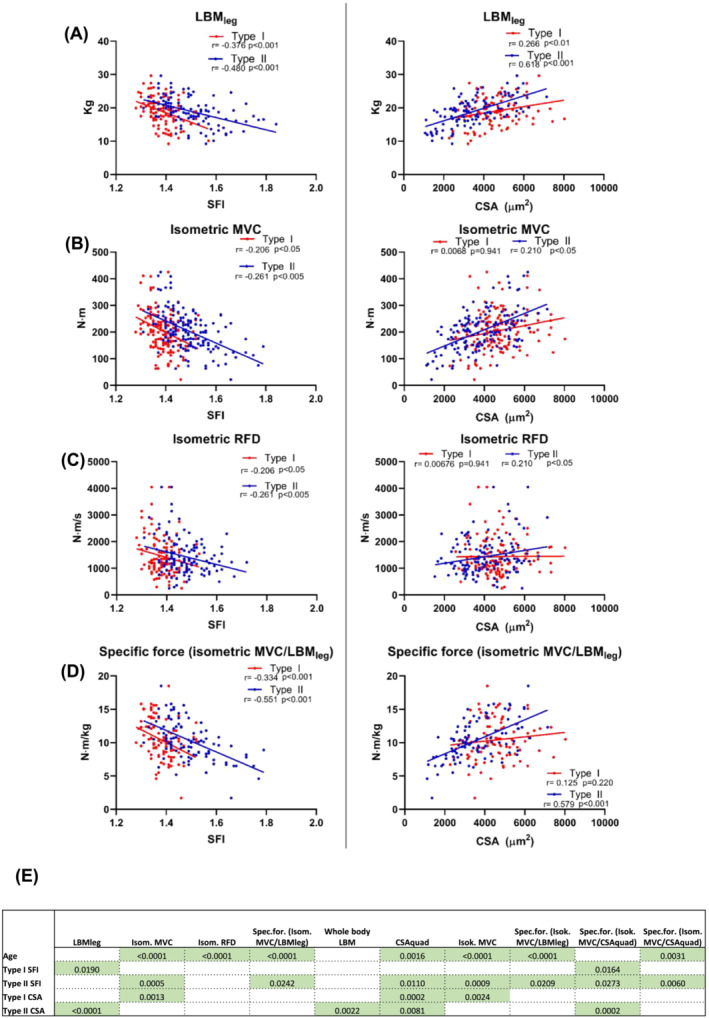
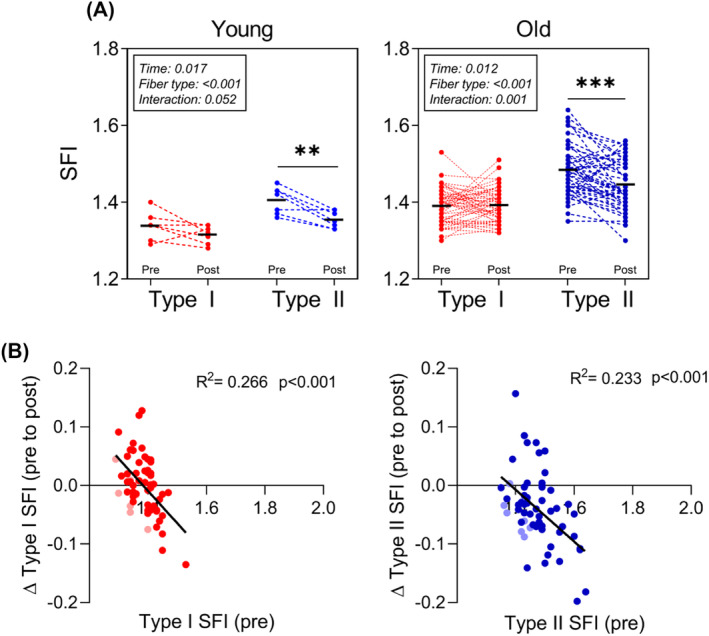
Results: In human muscle, SFI was positively correlated with age for both type I (R2 = 0.20) and II (R2 = 0.38) myofibers. When subjects were separated into age cohorts, SFI was lower for type I (4%, P < 0.001) and II (6%, P < 0.001) myofibers in young (20-36) compared with old (60-80) and higher for type I (5%, P < 0.05) and II (14%, P < 0.001) myofibers in the oldest old (>80) compared with old. The increased SFI in old muscle was observed in myofibers of all sizes. Within all three age cohorts, type II myofiber SFI was higher than that for type I myofiber (4-13%, P < 0.001), which was also the case in mice muscles (8-9%, P < 0.001). Across age cohorts, there was no difference between males and females in SFI for either type I (P = 0.496/0.734) or II (P = 0.176/0.585) myofibers. Multiple linear regression revealed that SFI, after adjusting for age and myofiber CSA, has independent explanatory power for 8/10 indices of muscle mass and function. RT reduced SFI of type II myofibers in both young and old (3-4%, P < 0.001).
Conclusions: Here, we identify type I and II myofiber shape in humans as a hallmark of muscle ageing that independently predicts volumetric and functional assessments of muscle health. RT reverts the shape of type II myofibers, suggesting that a lack of myofiber recruitment might lead to myofiber deformity.
Keywords: myofiber morphology; physiological function; sarcopenia; shape factor; skeletal muscle.
© 2023 The Authors. Journal of Cachexia, Sarcopenia and Muscle published by Wiley Periodicals LLC.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Tomlinson BE, Walton JN, Rebeiz JJ. The effects of ageing and of cachexia upon skeletal muscle. A histopathological study. J Neurol Sci 1969;9:321–346. - PubMed
-
- Lexell J, Taylor CC, Sjöström M. What is the cause of the ageing atrophy? Total number, size and proportion of different fiber types studied in whole vastus lateralis muscle from 15‐ to 83‐year‐old men. J Neurol Sci 1988;84:275–294. - PubMed
-
- Soendenbroe C, Heisterberg MF, Schjerling P, Karlsen A, Kjaer M, Andersen JL, et al. Molecular indicators of denervation in aging human skeletal muscle. Muscle Nerve 2019;60:453–463. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
