

Clinical-radiological-pathological correlation in pulmonary arterial hypertension
- PMID: 38123231
- PMCID: PMC10731450
- DOI: 10.1183/16000617.0138-2023
Clinical-radiological-pathological correlation in pulmonary arterial hypertension
Abstract
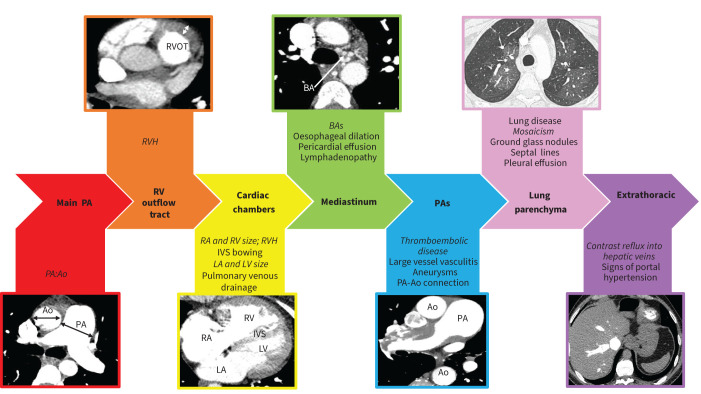
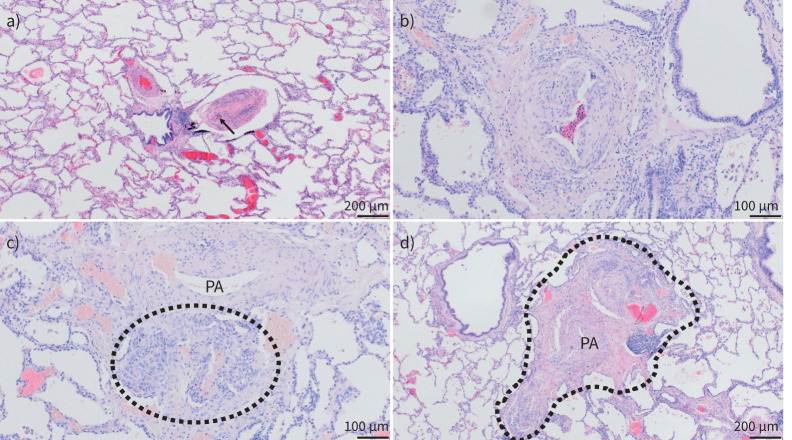
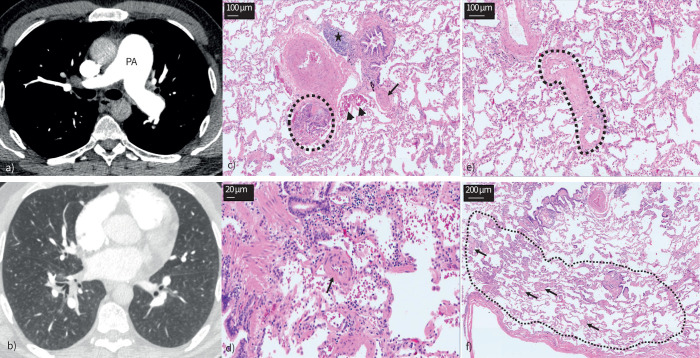
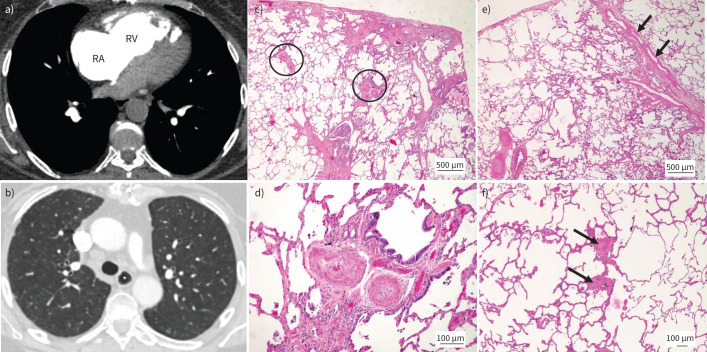
Pulmonary hypertension (PH) is defined by the presence of a mean pulmonary arterial pressure >20 mmHg. Current guidelines describe five groups of PH with shared pathophysiological and clinical features. In this paper, the first of a series covering all five PH classification groups, the clinical, radiological and pathological features of pulmonary arterial hypertension (PAH) will be reviewed. PAH may develop in the presence of associated medical conditions or a family history, following exposure to certain medications or drugs, or may be idiopathic in nature. Although all forms of PAH share common histopathological features, the presence of certain pulmonary arterial abnormalities, such as plexiform lesions, and extent of co-existing pulmonary venous involvement differs between the different subgroups. Radiological investigations are key to diagnosing the correct form of PH and a systematic approach to interpretation, especially of computed tomography, is essential.
Copyright ©The authors 2023.
Conflict of interest statement
Conflicts of interest: R. Condliffe, C. Durrington, A. Hameed, R.A. Lewis, R. Venkateswaran, D. Gopalan and P. Dorfmüller report no conflicts of interest related to this work.
Figures
Comment in
-
From the microscopic to the macroscopic: clinical-radiological-pathological correlation in pulmonary hypertension.Eur Respir Rev. 2023 Dec 20;32(170):230237. doi: 10.1183/16000617.0237-2023. Print 2023 Dec 31. Eur Respir Rev. 2023. PMID: 38123237 Free PMC article.
References
-
- European Respiratory Society . Pulmonary hypertension: clinical–radiological–pathological case series. Date last accessed: 8 July 2023. Date last updated: 31 March 2023. www.ersnet.org/events/pulmonary-hypertension-clinical-radiological-patho...
-
- Leber L, Beaudet A, Muller A. Epidemiology of pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension: identification of the most accurate estimates from a systematic literature review. Pulm Circ 2021; 11: 2045894020977300. doi: 10.1177/2045894020977300 - DOI - PMC - PubMed
-
- Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation 2010; 122: 164–172. doi: 10.1161/CIRCULATIONAHA.109.898122 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical