

A Population-Based and Clinical Cohort Validation of the Novel Consensus Definition of Metabolic Hyperferritinemia
- PMID: 38124275
- PMCID: PMC11099479
- DOI: 10.1210/clinem/dgad749
A Population-Based and Clinical Cohort Validation of the Novel Consensus Definition of Metabolic Hyperferritinemia
Abstract
Context: There is limited data on the clinical significance of metabolic hyperferritinemia (MHF) based on the most recent consensus.
Objective: We aimed to validate the clinical outcomes of MHF in the general population and patients with biopsy-proven metabolic dysfunction-associated fatty liver disease (MAFLD).
Methods: The NHANES database and PERSONS cohort were included. MHF was defined as elevated serum ferritin with metabolic dysfunction (MD) and stratified into different grades according to ferritin (grade 1: 200 [females]/300 [males]-550 ng/mL; grade 2: 550-1000 ng/mL; grade 3: >1000 ng/mL). The clinical outcomes, including all-cause death, comorbidities, and liver histology, were compared between non-MHF and MHF in adjusted models.
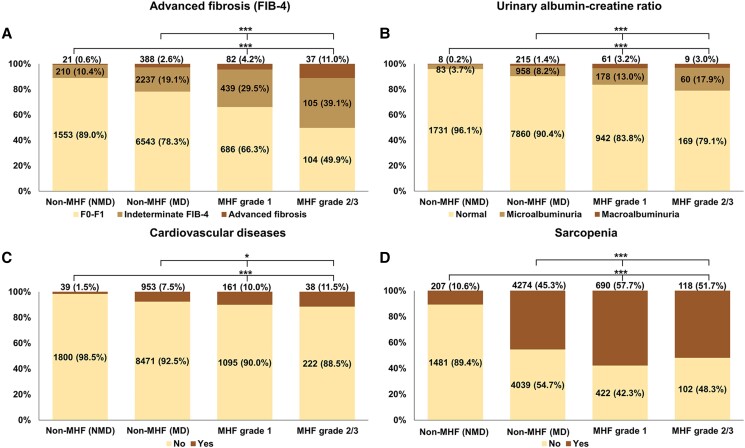
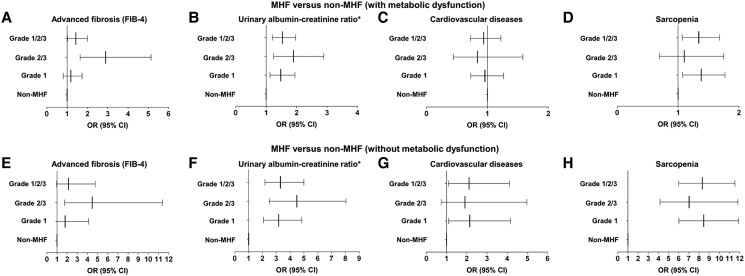
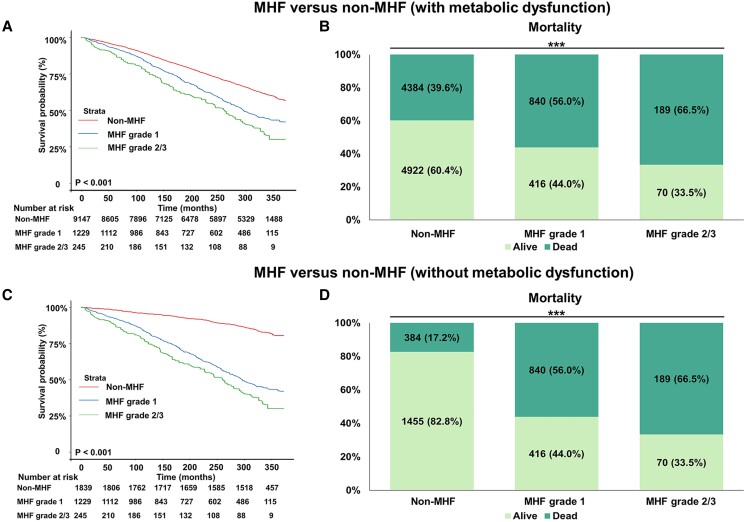
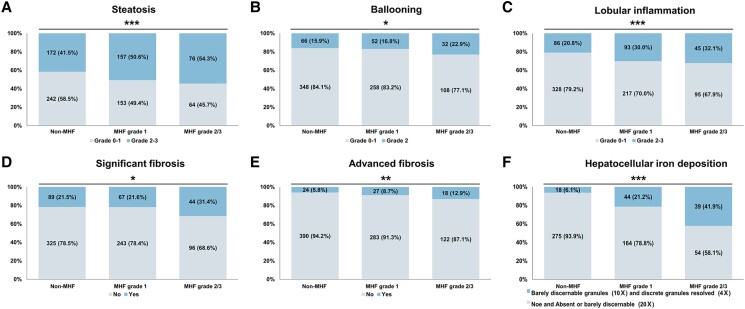
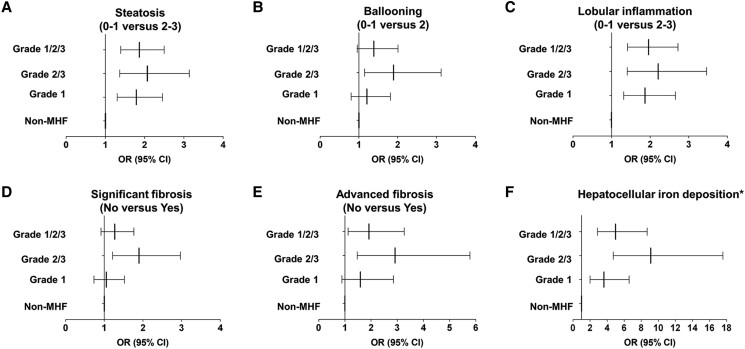
Results: In NHANES, compared with non-MHF with MD, MHF was related to higher risks of advanced fibrosis (P = .036), elevated albumin-creatinine ratio (UACR, P = .001), and sarcopenia (P = .013). Although the association between all grades of MHF and mortality was insignificant (P = .122), grades 2/3 was associated with increased mortality (P = .029). When comparing with non-MHF without MD, the harmful effects of MHF were more significant in mortality (P < .001), elevated UACR (P < .001), cardiovascular disease (P = .028), and sarcopenia (P < .001). In the PERSONS cohort, MHF was associated with more advanced grades of steatosis (P < .001), lobular inflammation (P < .001), advanced fibrosis (P = .017), and more severe hepatocellular iron deposition (P < .001).
Conclusion: Both in the general population and in at-risk individuals with MAFLD, MHF was related with poorer clinical outcomes.
Keywords: iron overload; metabolic dysfunction–associated fatty liver disease; metabolic hyperferritinemia; metabolic syndrome.
© The Author(s) 2023. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Joshi JG, Clauberg M. Ferritin: an iron storage protein with diverse functions. Biofactors. 1988;1(3):207‐212. - PubMed
-
- Aust SD. Ferritin as a source of iron and protection from iron-induced toxicities. Toxicol Lett. 1995;82–83:941‐944. - PubMed
-
- Cullis JO, Fitzsimons EJ, Griffiths WJ, et al. Investigation and management of a raised serum ferritin. Br J Haematol. 2018;181(3):331‐340. - PubMed
