

Evaluation of Safety and Efficacy of Preoperative Coronal MRI-Guided Minimally Invasive Surgery for Cervical Spondylotic Radiculopathy
- PMID: 38124352
- PMCID: PMC10750433
- DOI: 10.12659/MSM.942137
Evaluation of Safety and Efficacy of Preoperative Coronal MRI-Guided Minimally Invasive Surgery for Cervical Spondylotic Radiculopathy
Abstract
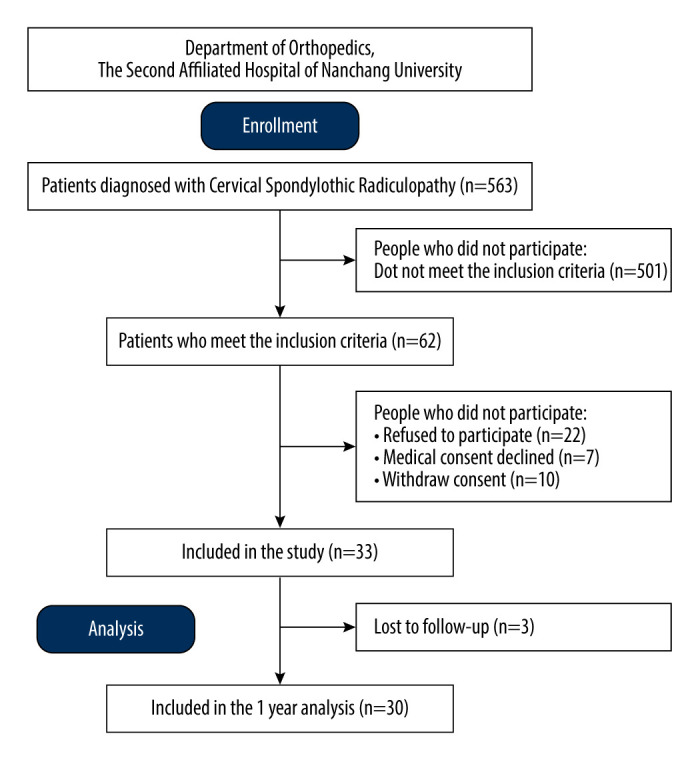
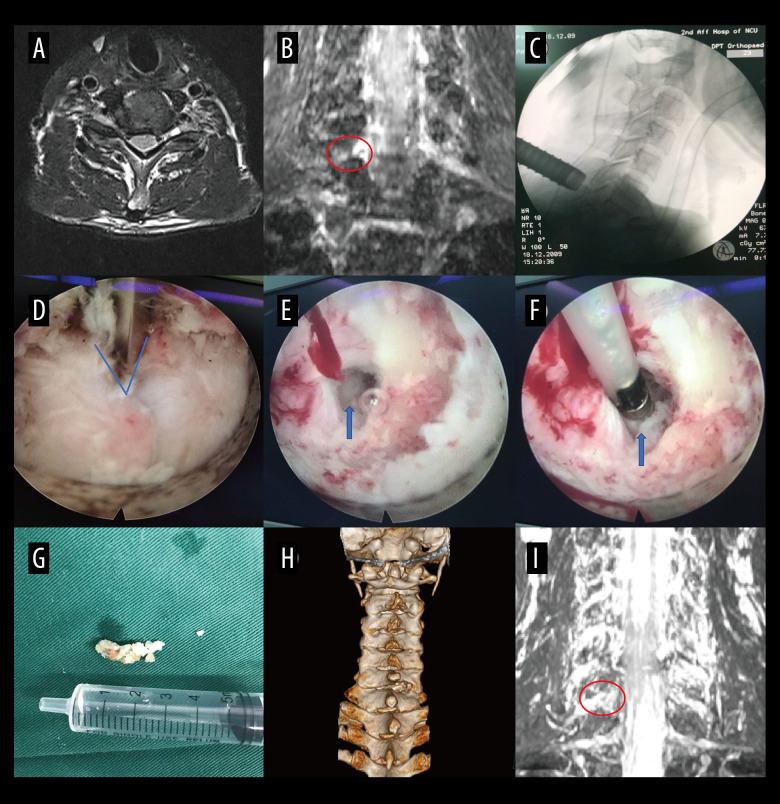
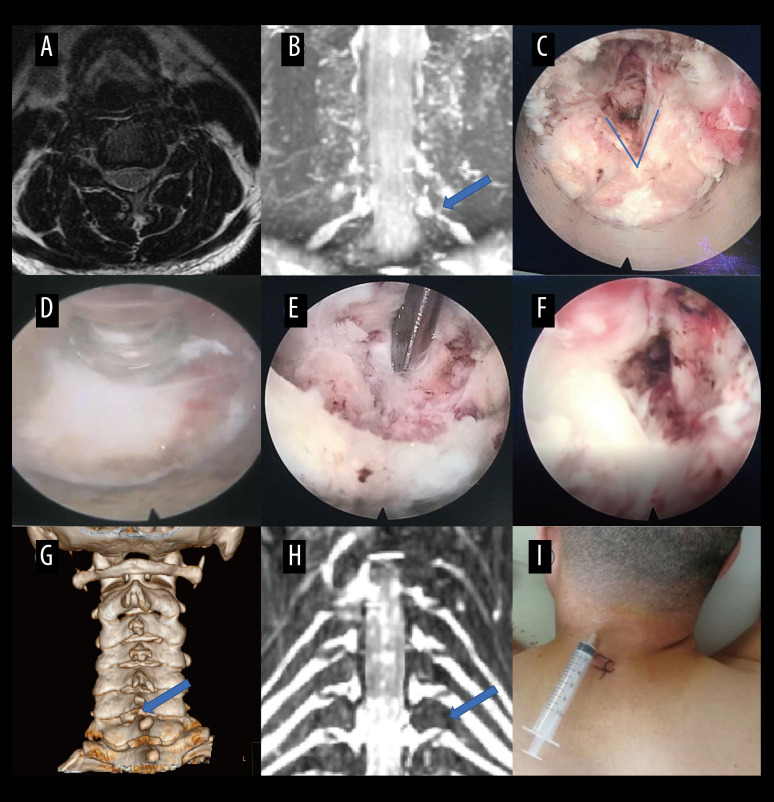
BACKGROUND Key-hole surgery is a minimally invasive technique that has shown promise in various surgical procedures. This study aimed to assess the clinical effectiveness of preoperative coronal MRI-assisted key-hole surgery for the treatment of patients with cervical spondylotic radiculopathy (CSR). MATERIAL AND METHODS A total of 30 patients diagnosed with CSR and undergoing key-hole surgery with CMRI assistance were included in the study. Various parameters, including surgical segments, incision length, disease duration, operative time, intraoperative fluoroscopy times, intraoperative blood loss, complications, and length of hospitalization, were recorded. Precise measurements of Cobb angles and intervertebral space height were taken before and after the surgical procedure. Surgical outcomes were evaluated using modified Macnab criteria, visual analogue scale (VAS), Japanese Orthopaedic Association Scores (JOA), and neck disability index (NDI). RESULTS The average duration of disease was 6.47±3.29 months, with an average incision length of 1.94±0.15 cm and operative time of 57.83±4.34 minutes. The average intraoperative blood loss was 33.70±9.28 ml, with an average of 3.50±0.73 intraoperative fluoroscopies. The average duration of hospitalization was 4.10±1.27 days. Preoperative and postoperative measurements showed no statistically significant difference in C2-C7 Cobb angles and intervertebral space height. However, there were significant improvements in postoperative VAS, NDI, and JOA scores compared to preoperative scores. The surgical effectiveness rate was 100%, with a high rate of good and excellent outcomes. CONCLUSIONS The findings of this study suggest that preoperative CMRI-assisted key-hole surgery for single-segment CSR is a safe and effective treatment option with low complication rates. The clinical benefits include high security and good outcomes. Further research and larger studies are warranted to validate these findings.
Conflict of interest statement
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
