

Obesity and hypertension: Obesity medicine association (OMA) clinical practice statement (CPS) 2023
- PMID: 38125655
- PMCID: PMC10728712
- DOI: 10.1016/j.obpill.2023.100083
Obesity and hypertension: Obesity medicine association (OMA) clinical practice statement (CPS) 2023
Abstract
Background: This Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) provides an overview of the mechanisms and treatment of obesity and hypertension.
Methods: The scientific support for this CPS is based upon published citations, clinical perspectives of OMA authors, and peer review by the Obesity Medicine Association leadership.
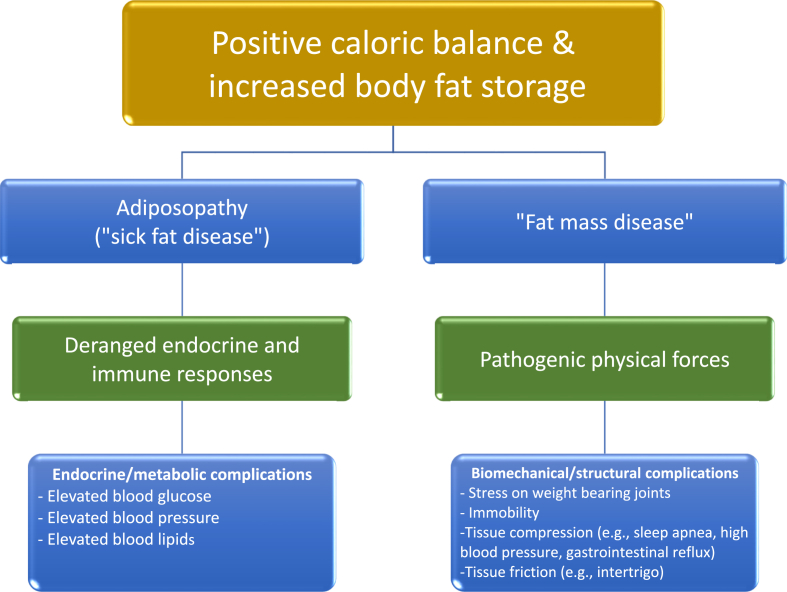
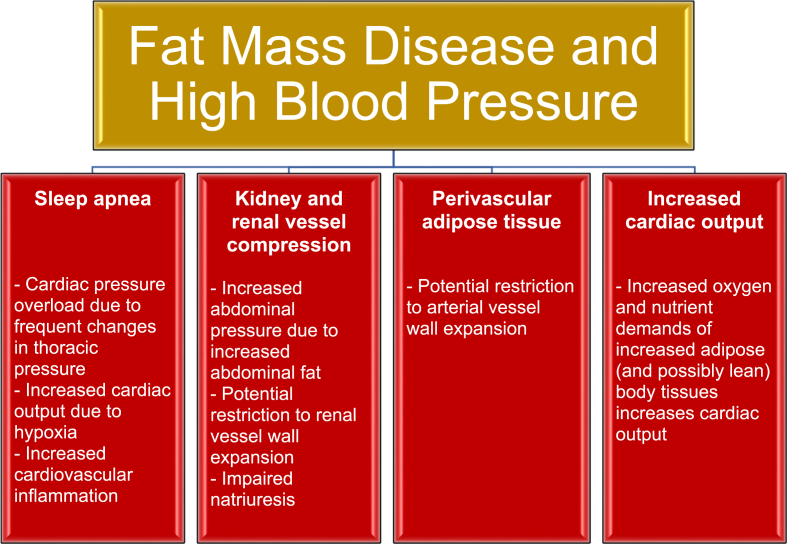
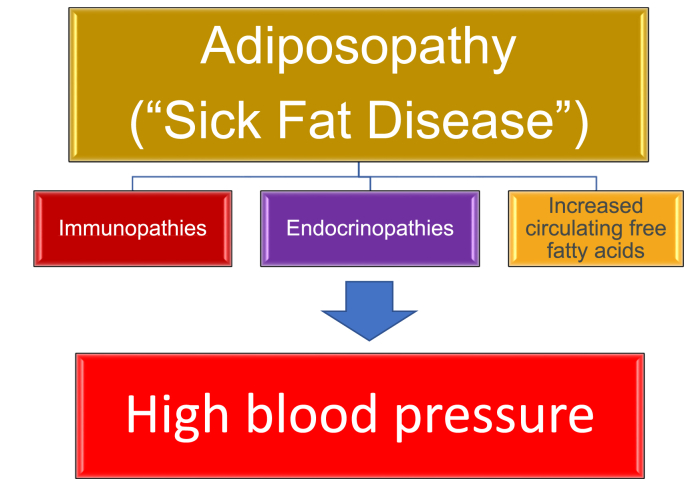
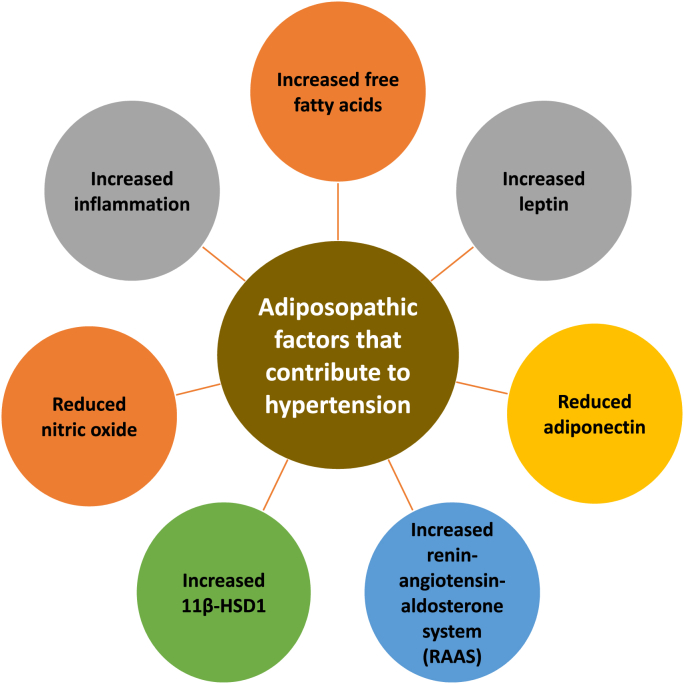
Results: Mechanisms contributing to obesity-related hypertension include unhealthful nutrition, physical inactivity, insulin resistance, increased sympathetic nervous system activity, renal dysfunction, vascular dysfunction, heart dysfunction, increased pancreatic insulin secretion, sleep apnea, and psychosocial stress. Adiposopathic factors that may contribute to hypertension include increased release of free fatty acids, increased leptin, decreased adiponectin, increased renin-angiotensin-aldosterone system activation, increased 11 beta-hydroxysteroid dehydrogenase type 1, reduced nitric oxide activity, and increased inflammation.
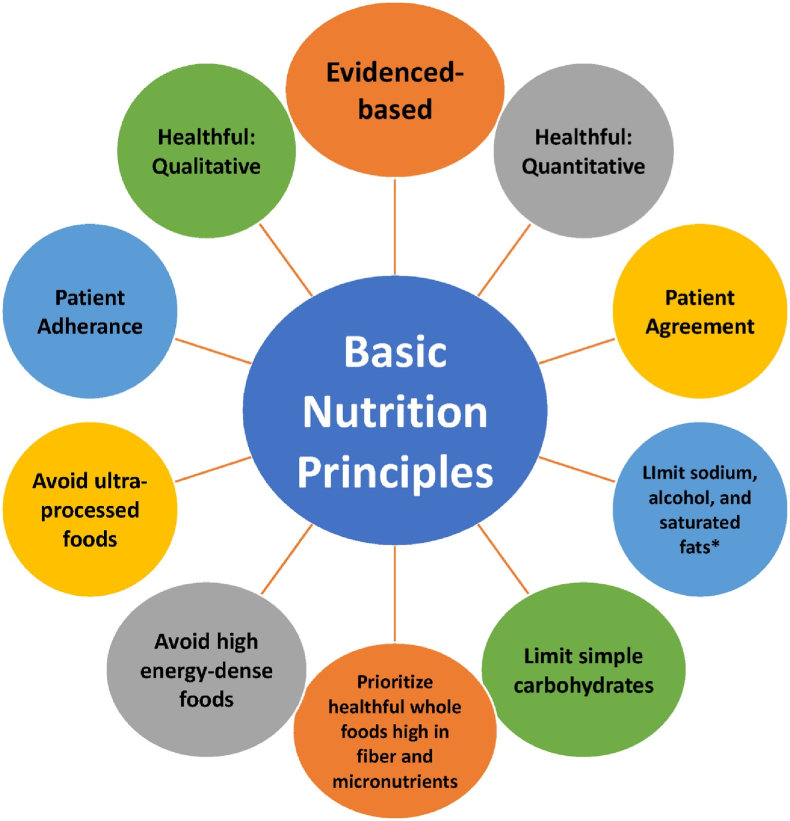
Conclusions: Increase in body fat is the most common cause of hypertension. Among patients with obesity and hypertension, weight reduction via healthful nutrition, physical activity, behavior modification, bariatric surgery, and anti-obesity medications mostly decrease blood pressure, with the greatest degree of weight reduction generally correlated with the greatest degree of blood pressure reduction.
Keywords: Adiposopathy; High blood pressure; Hypertension; Obesity.
© 2023 The Authors.
Figures

Similar articles
-
Obesity, thrombosis, venous disease, lymphatic disease, and lipedema: An obesity medicine association (OMA) clinical practice statement (CPS) 2023.Obes Pillars. 2023 Oct 19;8:100092. doi: 10.1016/j.obpill.2023.100092. eCollection 2023 Dec. Obes Pillars. 2023. PMID: 38125656 Free PMC article.
-
Obesity definition, diagnosis, bias, standard operating procedures (SOPs), and telehealth: An Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2022.Obes Pillars. 2022 Jan 15;1:100004. doi: 10.1016/j.obpill.2021.100004. eCollection 2022 Mar. Obes Pillars. 2022. PMID: 37990702 Free PMC article.
-
Bariatric surgery, gastrointestinal hormones, and the microbiome: An Obesity Medicine Association (OMA) Clinical Practice Statement (CPS) 2022.Obes Pillars. 2022 Apr 1;2:100015. doi: 10.1016/j.obpill.2022.100015. eCollection 2022 Jun. Obes Pillars. 2022. PMID: 37990718 Free PMC article.
-
Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms.Circ Res. 2015 Mar 13;116(6):991-1006. doi: 10.1161/CIRCRESAHA.116.305697. Circ Res. 2015. PMID: 25767285 Free PMC article. Review.
-
Obesity, dyslipidemia, and cardiovascular disease: A joint expert review from the Obesity Medicine Association and the National Lipid Association 2024.J Clin Lipidol. 2024 May-Jun;18(3):e320-e350. doi: 10.1016/j.jacl.2024.04.001. Epub 2024 Apr 24. J Clin Lipidol. 2024. PMID: 38664184 Review.
Cited by
-
Laser Acupuncture versus Liraglutide in Treatment of Obesity: A Multi-Institutional Retrospective Cohort Study.Healthcare (Basel). 2024 Jun 26;12(13):1279. doi: 10.3390/healthcare12131279. Healthcare (Basel). 2024. PMID: 38998814 Free PMC article.
-
An unbiased, sustainable, evidence-informed Universal Food Guide: a timely template for national food guides.Nutr J. 2024 Oct 18;23(1):126. doi: 10.1186/s12937-024-01018-z. Nutr J. 2024. PMID: 39425106 Free PMC article. Review.
-
Exploring the nonlinear relationship between serum uric acid to high-density lipoprotein cholesterol ratio and obesity in older adults: a cross-sectional study.Front Public Health. 2025 May 1;13:1587194. doi: 10.3389/fpubh.2025.1587194. eCollection 2025. Front Public Health. 2025. PMID: 40376050 Free PMC article.
-
Obesity, thrombosis, venous disease, lymphatic disease, and lipedema: An obesity medicine association (OMA) clinical practice statement (CPS) 2023.Obes Pillars. 2023 Oct 19;8:100092. doi: 10.1016/j.obpill.2023.100092. eCollection 2023 Dec. Obes Pillars. 2023. PMID: 38125656 Free PMC article.
-
Effects of Increasing Farmed Salmon Intake to the Recommended Fish-Intake Amounts on Lipid Profile in Young Women: An 8-Week Intervention Study.Nutrients. 2024 Nov 26;16(23):4051. doi: 10.3390/nu16234051. Nutrients. 2024. PMID: 39683444 Free PMC article. Clinical Trial.
References
-
- Bays HE, McCarthy W, Burridge K, Tondt J, Karjoo S, Christensen S, Ng J, Golden A, Davisson L, Richardson L. Obesity Algorithm eBook, presented by the obesity medicine association. www.obesityalgorithm.org. 2021. https://obesitymedicine.org/obesity-algorithm/.
-
- Rizzoni D. Masked hypertension: how to identify and when to treat? High Blood Pres Cardiovasc Prev. 2016;23:181–186. - PubMed
-
- Peters G.L., Binder S.K., Campbell N.R. The effect of crossing legs on blood pressure: a randomized single-blind cross-over study. Blood Press Monit. 1999;vol. 4:97–101. - PubMed
LinkOut - more resources
Full Text Sources
