

A practical approach to the diagnosis and management of malignant pleural effusions in resource-constrained settings
- PMID: 38125800
- PMCID: PMC10729815
- DOI: 10.1183/20734735.0140-2023
A practical approach to the diagnosis and management of malignant pleural effusions in resource-constrained settings
Abstract
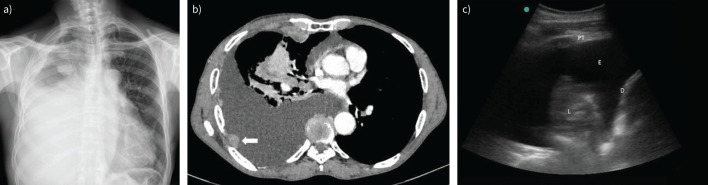
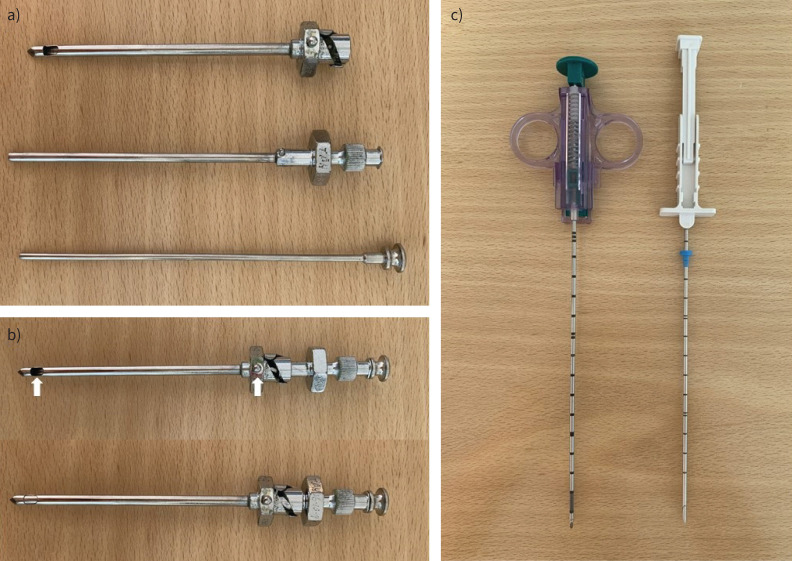
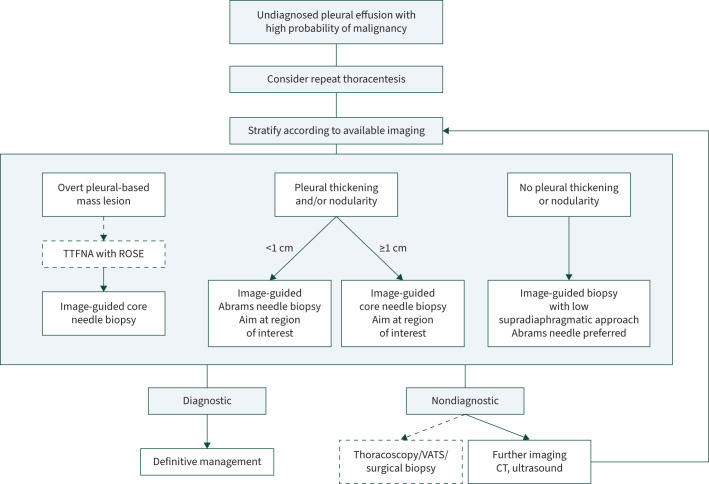
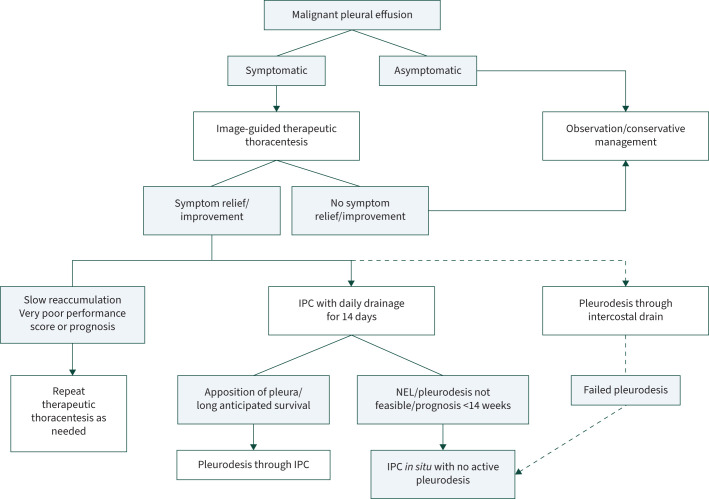
No pleural intervention in a patient with confirmed malignant pleural effusion (MPE) prolongs life, but even the recommended interventions for diagnosis and palliation can be costly and therefore unavailable in large parts of the world. However, there is good evidence to guide clinicians working in low- and middle-income countries on the most cost-effective and clinically effective strategies for the diagnosis and management of MPE. Transthoracic ultrasound-guided closed pleural biopsy is a safe method of pleural biopsy with a diagnostic yield approaching that of thoracoscopy. With the use of pleural fluid cytology and ultrasound-guided biopsy, ≥90% of cases can be diagnosed. Cases with an associated mass lesion are best suited to an ultrasound-guided fine needle aspiration with/without core needle biopsy. Those with diffuse pleural thickening and/or nodularity should have an Abrams needle (<1 cm thickening) or core needle (≥1 cm thickening) biopsy of the area of interest. Those with insignificant pleural thickening should have an ultrasound-guided Abrams needle biopsy close to the diaphragm. The goals of management are to alleviate dyspnoea, prevent re-accumulation of the pleural effusion and minimise re-admissions to hospital. As the most cost-effective strategy, we suggest early use of indwelling pleural catheters with daily drainage for 14 days, followed by talc pleurodesis if the lung expands. The insertion of an intercostal drain with talc slurry is an alternative strategy which is noninferior to thoracoscopy with talc poudrage.
Educational aims: To provide clinicians practising in resource-constrained settings with a practical evidence-based approach to the diagnosis and management of malignant pleural effusions.To explain how to perform an ultrasound-guided closed pleural biopsy.To explain the cost-effective use of indwelling pleural catheters.
Copyright ©ERS 2023.
Conflict of interest statement
Conflict of interest: J.A. Shaw reports receiving an honorarium from AstraZeneca, outside the submitted work. E.H. Louw has nothing to disclose. C.F.N. Koegelenberg reports receiving an honorarium from GSK and AstraZeneca, outside the submitted work.
Figures

Comment in
- doi: 10.1183/20734735.0230-2023
References
-
- Ebrahimi H, Aryan Z, Saeedi Moghaddam S, et al. . Global, regional, and national burden of respiratory tract cancers and associated risk factors from 1990 to 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Respir Med 2021; 9: 1030–1049. doi:10.1016/S2213-2600(21)00164-8 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials