

Predictive Model of All-Cause Death in Patients with Heart Failure using Heart Rate Variability
- PMID: 38126484
- PMCID: PMC10763696
- DOI: 10.36660/abc.20220379
Predictive Model of All-Cause Death in Patients with Heart Failure using Heart Rate Variability
Abstract
Background: Central Illustration : Predictive Model of All-Cause Death in Patients with Heart Failure using Heart Rate Variability.
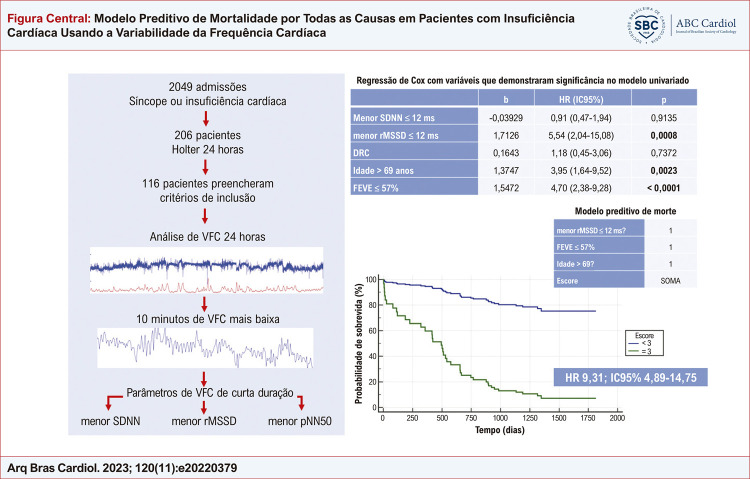
Background: Short and long-duration heart rate variability (HRV) data from Holter monitoring could identify predictors of all-cause death in heart failure (HF) patients.
Objectives: To build a predictive model of all-cause death in patients with HF using HRV.
Methods: Retrospective study including patients with suspected or confirmed HF who were admitted for decompensated HF or syncope that underwent Holter monitoring. In analysis of augmented sympathetic tonus, we evaluated the lowest HRV in nonoverlapping 10-minutes periods throughout 24h continuous electrocardiographic signal recording (short HRV variables). Variables with p<0.01 were included in a multivariate Cox regression model to determine the occurrence of the all-cause death. Variables with statistical significance in Cox regression were chosen to build the predictive model. P<0.05 was considered significant.
Results: A total of 116 patients were included, mean age of 71.9±16.3 years, 45.7% men, mean follow-up of 2.83±1.27 years. Thirty-nine deaths occurred (33.6%). By comparing survivors vs. non-survivors, the variables that showed statistical significance were lowest SDNN, lowest rMSSD, age and left ventricular ejection fraction (LVEF). In Cox regression, independent predictors of all-cause death were: age>69 years (HR 3.95, 95%CI 1.64-9.52); LVEF≤57% (HR 4.70, 95%CI 2.38-9.28) and lowest rMSSD≤12ms (HR 5.54, 95%CI 2.04-15.08). An integer value was assigned to each variable. Score<3 showed AUC=0.802 (95%CI 0.72-0.87).
Conclusion: In HF patients hospitalized for decompensated HF or syncope, independent long-term predictors of all-cause death were age, LVEF, and 10-minutes rMSSD. These findings indicate that even brief moments of high sympathetic tone can impact survival, specifically in the elderly and patients with HF with reduced ejection fraction.
Figura Central : Modelo Preditivo de Mortalidade por Todas as Causas em Pacientes com Insuficiência Cardíaca Usando a Variabilidade da Frequência Cardíaca.
Fundamento: Dados de curto e de longo prazo da variabilidade da frequência cardíaca (VFC) poderiam identificar preditores de mortalidade por todas as causas em pacientes com insuficiência cardíaca (IC).
Objetivos: Construir um modelo preditivo de mortalidade por todas as causas em pacientes com IC usando a VFC.
Métodos: Estudo retrospectivo incluindo pacientes com suspeita ou diagnóstico confirmado de IC internados por IC descompensada ou síncope e que realizaram exame de Holter 24 horas. Na análise do tônus simpático aumentado, nós avaliamos a VFC mais baixa em períodos de 10 minutos não sobrepostos em um registro contínuo de sinal eletrocardiográfico por 24 horas (VFC de curta duração). As variáveis com p<0,01 foram incluídas no modelo de regressão multivariada de Cox para determinar a ocorrência da mortalidade por todas as causas. As variáveis com significância estatística na regressão de Cox foram escolhidas para construir o modelo preditivo. Um p<0,05 foi considerado estatisticamente significativo.
Resultados: Um total de 116 pacientes foram incluídos, com idade média de 71,9±16,3 anos, 45,7% eram do sexo masculino. O tempo médio de acompanhamento foi de 2,83 ± 1,27 anos. Trinta e nove (33,6%) óbitos ocorreram. Na comparação de sobreviventes e não sobreviventes, as variáveis que mostraram significância estatística foram menor SDNN, menor rMSSD, idade e fração de ejeção ventricular esquerda (FEVE). Na regressão Cox, os preditores independentes de mortalidade por todas as causas foram: idade > 69 anos (HR 3,95, IC95% 1,64-9,52); FEVE≤57% (HR 4,70, IC95% 2,38-9,28) e menor rMSSD ≤12ms (HR 5,54; IC 95% 2,04-15,08). Um valor inteiro foi atribuído para cada variável. Este escore < 3 apresentou uma área sob a curva de 0,802 (IC95% 0,72-0,87).
Conclusão: Em pacientes com IC internados por IC descompensada ou síncope, preditores de longo prazo de mortalidade por todas as causas foram idade, FEVE, e rMSSD em 10 minutos. Esses achados indicam que mesmo breves momentos de tônus simpático elevado podem ter impacto na sobrevida, principalmente em idosos e pacientes com IC e fração de ejeção reduzida.
Conflict of interest statement
Potencial conflito de interesse
Não há conflito com o presente artigo
Figures




References
-
- Schwartz PJ, La Rovere MT, Vanoli E. Autonomic Nervous System and Sudden Cardiac Death. Experimental Basis and Clinical Observations for Post-Myocardial Infarction Risk Stratification. Circulation. 1992;85(1) Suppl:I77–I91. - PubMed
-
- Heart Rate Variability Standards of Measurement, Physiological Interpretation, and Clinical Use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Eur Heart J. 1996;17(3):354–381. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
