

Impact of repeat ablation of ventricular tachycardia in patients with structural heart disease
- PMID: 38127308
- PMCID: PMC10755192
- DOI: 10.1093/europace/euad367
Impact of repeat ablation of ventricular tachycardia in patients with structural heart disease
Abstract
Aims: Recurrences of ventricular tachycardia (VT) after initial catheter ablation is a significant clinical problem. In this study, we report the efficacy and risks of repeat VT ablation in patients with structural heart disease (SHD) in a tertiary single centre over a 7-year period.
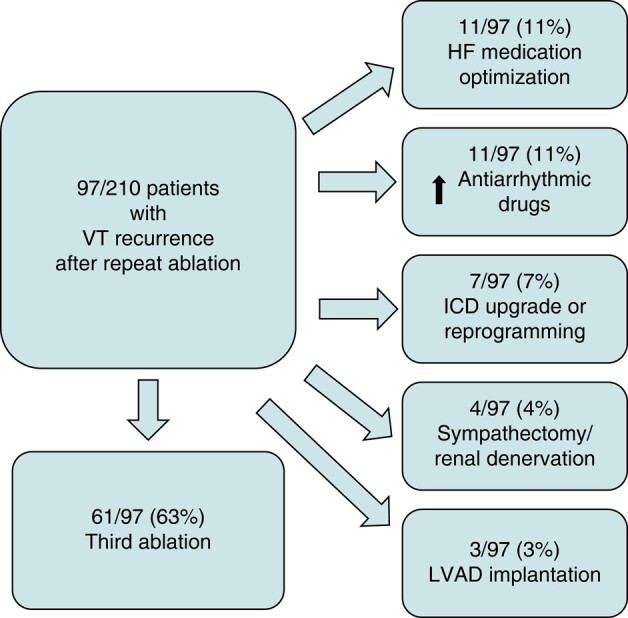
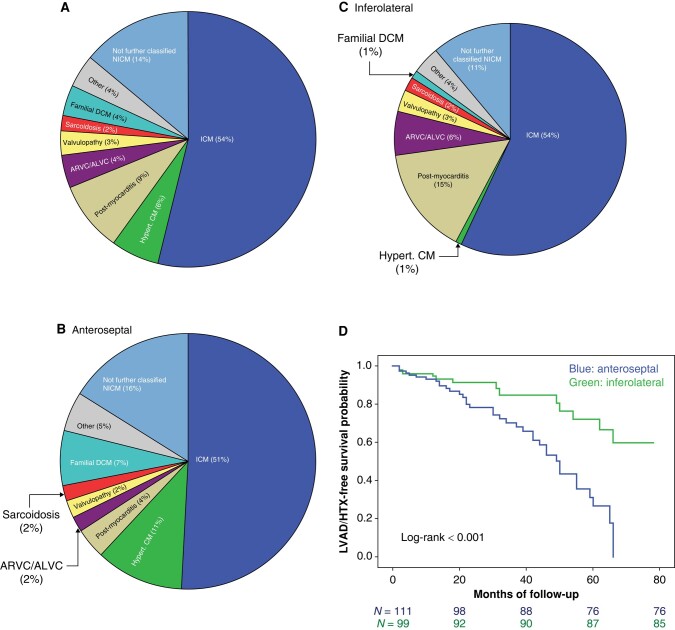
Methods and results: Two hundred ten consecutive patients referred for repeat VT ablation after previous ablation in our institution were included in the analysis (53% ischaemic cardiomyopathy, 91% males, median age 65 years, mean left ventricular ejection fraction 35%). After performing repeat ablation, the clinical VTs were acutely eliminated in 82% of the patients, but 46% of the cohort presented with VT recurrence during the 25-month follow-up. Repeat ablation led to a 73% reduction of shock burden in the first year and 61% reduction until the end of follow-up. Similarly, VT burden was reduced 55% in the first year and 36% until the end of the study. Fifty-two patients (25%) reached the combined endpoint of ventricular assist device implantation, heart transplantation, or death. Advanced New York Heart Association functional class, anteroseptal substrate, and periprocedural complication after repeat ablation were associated with worse prognosis independently of the type of cardiomyopathy.
Conclusion: While complete freedom from VT after repeat ablation in SHD was difficult to achieve, ablation led to a significant reduction in VT and shock burden. Besides advanced heart failure characteristics, anteroseptal substrate and periprocedural complications predicted a worse outcome.
Keywords: Acute and long-term freedom from VT; Prognosis after repeat VT ablation; Repeat ablation in ventricular arrhythmias; Risks and complication management.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: none declared.
Figures


Similar articles
-
Epicardial ablation of ventricular tachycardia in patients with structural heart disease: a single-centre experience over 12 years.Europace. 2021 Dec 7;23(12):1980-1988. doi: 10.1093/europace/euab194. Europace. 2021. PMID: 34405874
-
Long-term outcomes after catheter ablation of ventricular tachycardia in patients with and without structural heart disease.Heart Rhythm. 2016 Oct;13(10):1957-63. doi: 10.1016/j.hrthm.2016.07.001. Epub 2016 Jul 5. Heart Rhythm. 2016. PMID: 27392945
-
Gender differences in patients with structural heart disease undergoing VT ablation.J Cardiovasc Electrophysiol. 2021 Oct;32(10):2675-2683. doi: 10.1111/jce.15219. Epub 2021 Aug 24. J Cardiovasc Electrophysiol. 2021. PMID: 34411387
-
Catheter ablation as first-line treatment for ventricular tachycardia in patients with structural heart disease and preserved left ventricular ejection fraction: a systematic review and meta-analysis.Sci Rep. 2024 Aug 9;14(1):18536. doi: 10.1038/s41598-024-69467-4. Sci Rep. 2024. PMID: 39122752 Free PMC article.
-
Catheter Ablation for Ventricular Tachycardia in Ischaemic Versus Non-Ischaemic Cardiomyopathy: A Systematic Review and Meta-Analysis.Heart Lung Circ. 2022 Aug;31(8):1064-1074. doi: 10.1016/j.hlc.2022.02.014. Epub 2022 May 25. Heart Lung Circ. 2022. PMID: 35643798
Cited by
-
Personalized Heart Digital Twins Detect Substrate Abnormalities in Scar-Dependent Ventricular Tachycardia.Circulation. 2025 Feb 25;151(8):521-533. doi: 10.1161/CIRCULATIONAHA.124.070526. Epub 2025 Jan 6. Circulation. 2025. PMID: 39758009
-
Ventricular Intramyocardial Navigation for Tachycardia Ablation Guided by Electrograms (VINTAGE): Initial Human Experience.JACC Clin Electrophysiol. 2025 Jul 7:S2405-500X(25)00462-1. doi: 10.1016/j.jacep.2025.06.003. Online ahead of print. JACC Clin Electrophysiol. 2025. PMID: 40704960
-
Percutaneous mechanical support in catheter ablation of ventricular arrhythmias: hype or hope?Europace. 2024 Jul 2;26(7):euae186. doi: 10.1093/europace/euae186. Europace. 2024. PMID: 39028767 Free PMC article. Review.
-
Pre-ablation and Post-ablation Factors Influencing the Prognosis of Patients with Electrical Storm Treated by Radiofrequency Catheter Ablation: An Update.Rev Cardiovasc Med. 2024 Dec 5;25(12):432. doi: 10.31083/j.rcm2512432. eCollection 2024 Dec. Rev Cardiovasc Med. 2024. PMID: 39742218 Free PMC article. Review.
-
Optimizing ventricular tachycardia ablation through imaging-based assessment of arrhythmic substrate: A comprehensive review and roadmap for the future.Heart Rhythm O2. 2024 Jul 5;5(8):561-572. doi: 10.1016/j.hroo.2024.07.001. eCollection 2024 Aug. Heart Rhythm O2. 2024. PMID: 39263615 Free PMC article. Review.
References
-
- Kuck KH, Tilz RR, Deneke T, Hoffmann BA, Ventura R, Hansen PS et al. Impact of substrate modification by catheter ablation on implantable cardioverter-defibrillator interventions in patients with unstable ventricular arrhythmias and coronary artery disease: results from the multicenter randomized controlled SMS (Substrate Modification Study). Circ Arrhythm Electrophysiol 2017;10:e004422. - PubMed
-
- Kuck KH, Schaumann A, Eckardt L, Willems S, Ventura R, Delacrétaz E et al. Catheter ablation of stable ventricular tachycardia before defibrillator implantation in patients with coronary heart disease (VTACH): a multicentre randomised controlled trial. Lancet 2010;375:31–40. - PubMed
-
- Zeppenfeld K, Tfelt-Hansen J, De Riva M, Winkel BG, Behr ER, Blom NA et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J 2022;43:3997–4126. - PubMed
-
- Dinov B, Fiedler L, Schönbauer R, Bollmann A, Rolf S, Piorkowski C et al. Outcomes in catheter ablation of ventricular tachycardia in dilated non-ischemic cardiomyopathy in comparison to ischemic cardiomyopathy: results from the Prospective Heart Centre of Leipzig VT (HELP-VT) study. Circulation 2014;129:728–36. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
