

Whole-Brain Radiotherapy Alone vs Preceded by Bevacizumab, Etoposide, and Cisplatin for Untreated Brain Metastases From Breast Cancer: A Randomized Clinical Trial
- PMID: 38127335
- PMCID: PMC10739128
- DOI: 10.1001/jamaoncol.2023.5456
Whole-Brain Radiotherapy Alone vs Preceded by Bevacizumab, Etoposide, and Cisplatin for Untreated Brain Metastases From Breast Cancer: A Randomized Clinical Trial
Abstract
Importance: The incidence of brain metastasis is increasing in patients with metastatic breast cancer. Treatments to extend the control of brain metastasis are urgently required.
Objective: To investigate whether the addition of an induction treatment of bevacizumab, etoposide, and cisplatin (BEEP) improves brain-specific progression-free survival (PFS) after whole-brain radiotherapy (WBRT).
Design, setting, and participants: This open-label, randomized, multicenter clinical trial assessed patients with brain metastases from breast cancer (BMBC) in Taiwan from September 9, 2014, to December 24, 2018, with survival follow-up until December 31, 2021. Key inclusion criteria included metastatic brain tumors not suitable for focal treatment, WBRT naivety, age 20 to 75 years, and at least 1 measurable brain metastatic lesion. The primary end point was brain-specific PFS, with an expected hazard ratio of 0.60, a 2-sided α ≤ .20, and power of 0.8.
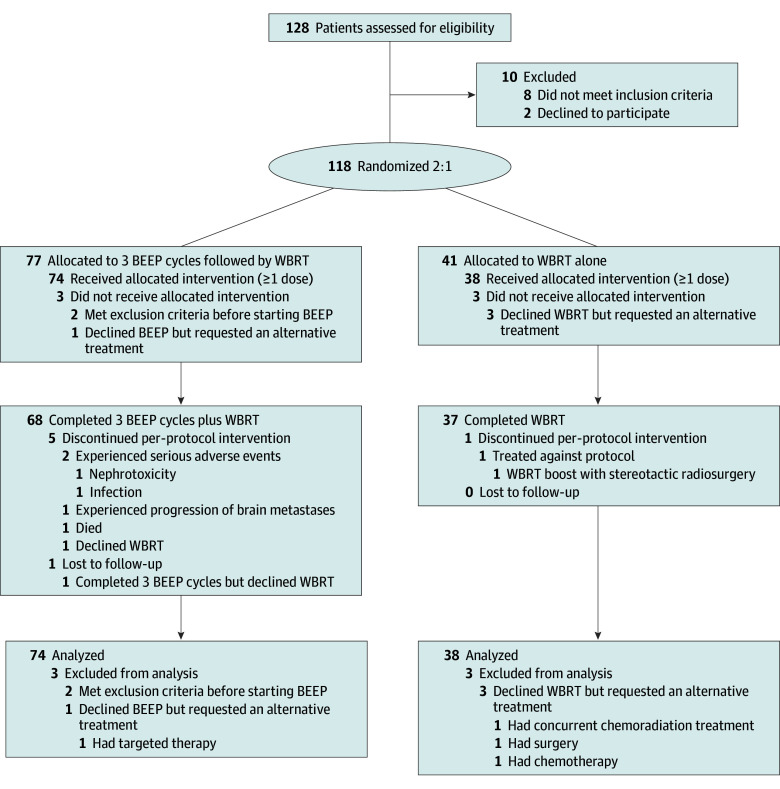
Interventions: Eligible patients were randomly assigned at a ratio of 2:1 to the experimental arm, which involved 3 cycles of BEEP followed by WBRT, or the control arm, which involved WBRT alone.
Main outcomes and measures: The primary end point was the determination of brain-specific PFS by local investigators according to the Response Evaluation Criteria in Solid Tumors, version 1.1, the initiation of other brain-directed treatment after WBRT, or death. Other key end points included brain-specific objective response rate after 8 weeks of BEEP treatment or WBRT and 8-month brain-specific PFS rate, PFS, and overall survival.
Results: A total of 118 patients with BMBC were randomized, with the intention-to-treat cohort comprising 112 patients. The median age was 56 years (range, 34-71 years), and 61 patients (54.5%) had ERBB2 (formerly HER2 or HER2/neu)-positive disease. The median (range) brain-specific PFS was 8.1 (0.3-29.5) vs 6.5 (0.9-25.5) months in the experimental and control arms, respectively (hazard ratio, 0.71; 95% CI, 0.44-1.13; P = .15; significant at predefined α ≤ .20). The brain-specific objective response rate at 2 months was not significantly different (BEEP treatment vs WBRT, 41.9% vs 52.6%), but the 8-month brain-specific PFS rate was significantly higher in the experimental group (48.7% vs 26.3%; P = .03). Adverse events were generally manageable with prophylactic granulocyte colony-stimulating factor treatment.
Conclusions and relevance: The findings show that induction BEEP before WBRT may improve the control of BMBC compared with using upfront WBRT, which could address an unmet need for an effective systemic treatment for intractable brain and extracranial metastases from metastatic breast cancer.
Trial registration: ClinicalTrials.gov Identifier: NCT02185352.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
