

Abandonment of Routine Radiotherapy for Nonlocally Advanced Rectal Cancer and Oncological Outcomes
- PMID: 38127337
- PMCID: PMC10739079
- DOI: 10.1001/jamaoncol.2023.5444
Abandonment of Routine Radiotherapy for Nonlocally Advanced Rectal Cancer and Oncological Outcomes
Abstract
Importance: Neoadjuvant short-course radiotherapy was routinely applied for nonlocally advanced rectal cancer (cT1-3N0-1M0 with >1 mm distance to the mesorectal fascia) in the Netherlands following the Dutch total mesorectal excision trial. This policy has shifted toward selective application after guideline revision in 2014.
Objective: To determine the association of decreased use of neoadjuvant radiotherapy with cancer-related outcomes and overall survival at a national level.
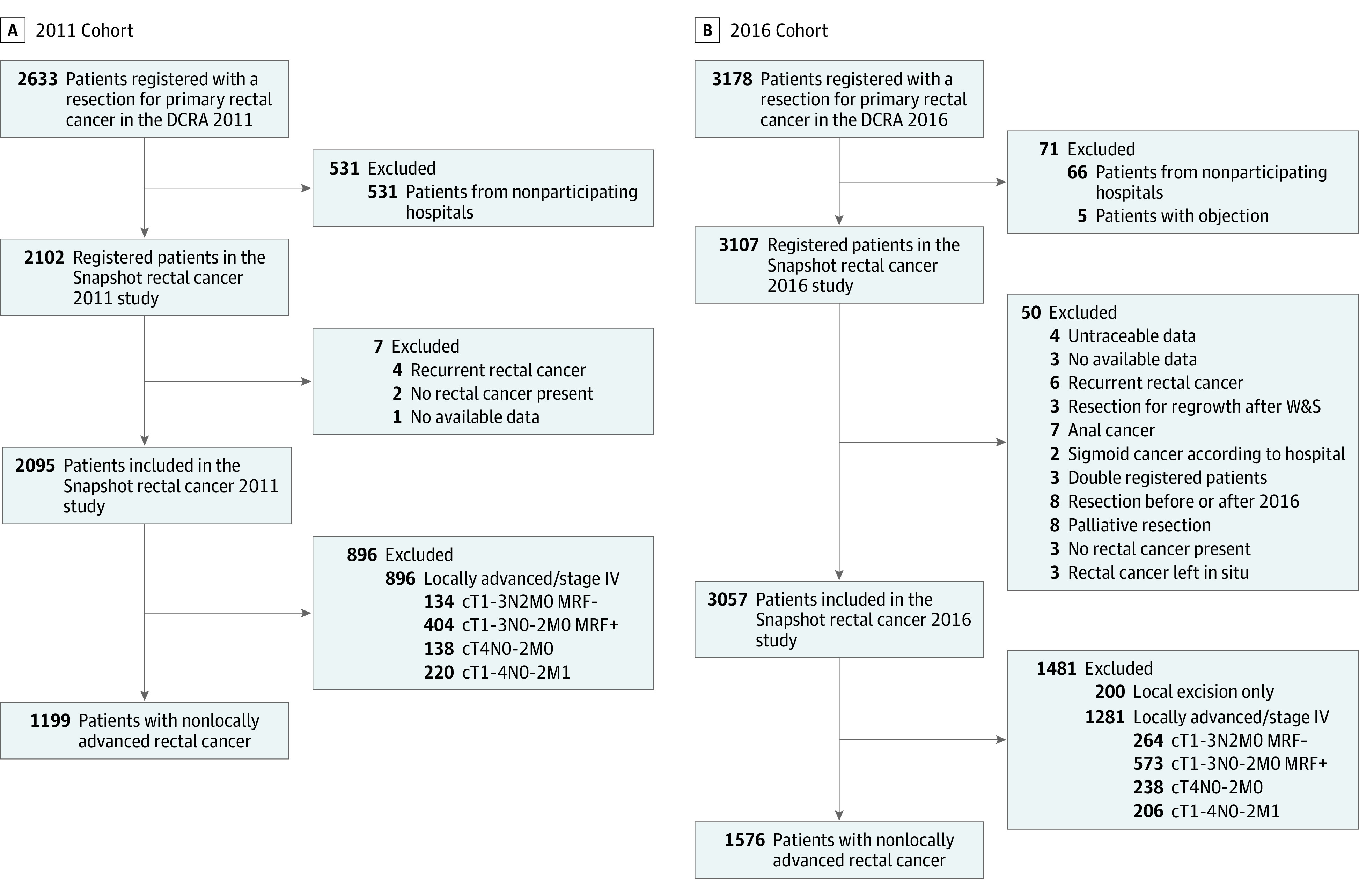
Design, setting, and participants: This multicenter, population-based, nationwide cross-sectional cohort study analyzed Dutch patients with rectal cancer who were treated in 2011 with a 4-year follow-up. A similar study was performed in 2021, analyzing all patients that were surgically treated in 2016. From these cohorts, all patients with cT1-3N0-1M0 rectal cancer and radiologically unthreatened mesorectal fascia were included in the current study. The data of the 2011 cohort were collected between May and October 2015, and the data of the 2016 cohort were collected between October 2020 and November 2021. The data were analyzed between May and October 2022.
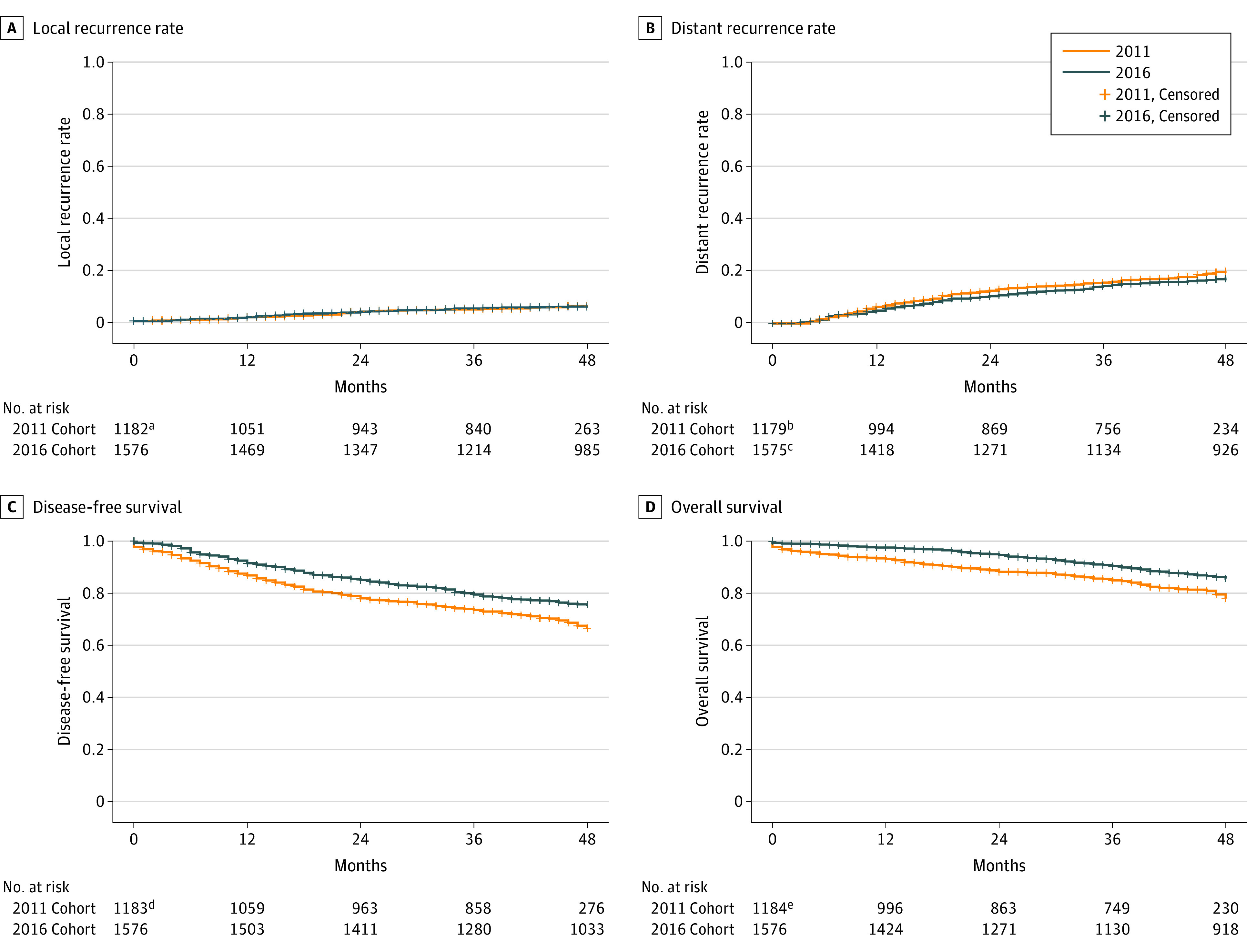
Main outcomes and measures: The main outcomes were 4-year local recurrence and overall survival rates.
Results: Among the 2011 and 2016 cohorts, 1199 (mean [SD] age, 68 [11] years; 430 women [36%]) of 2095 patients (57.2%) and 1576 (mean [SD] age, 68 [10] years; 547 women [35%]) of 3057 patients (51.6%) had cT1-3N0-1M0 rectal cancer and were included, with proportions of neoadjuvant radiotherapy of 87% (2011) and 37% (2016). Four-year local recurrence rates were 5.8% and 5.5%, respectively (P = .99). Compared with the 2011 cohort, 4-year overall survival was significantly higher in the 2016 cohort (79.6% vs 86.4%; P < .001), with lower non-cancer-related mortality (13.8% vs 6.3%; P < .001).
Conclusions and relevance: The results of this cross-sectional study suggest that an absolute 50% reduction in radiotherapy use for nonlocally advanced rectal cancer did not compromise cancer-related outcomes at a national level. Optimizing clinical staging and surgery following the Dutch total mesorectal excision trial has potentially enabled safe deintensification of treatment.
Conflict of interest statement
Figures
References
-
- van Gijn W, Marijnen CA, Nagtegaal ID, et al. ; Dutch Colorectal Cancer Group . Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011;12(6):575-582. doi:10.1016/S1470-2045(11)70097-3 - DOI - PubMed
-
- Sebag-Montefiore D, Stephens RJ, Steele R, et al. . Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): a multicentre, randomised trial. Lancet. 2009;373(9666):811-820. doi:10.1016/S0140-6736(09)60484-0 - DOI - PMC - PubMed
-
- Marijnen CA, Kapiteijn E, van de Velde CJ, et al. ; Cooperative Investigators of the Dutch Colorectal Cancer Group . Acute side effects and complications after short-term preoperative radiotherapy combined with total mesorectal excision in primary rectal cancer: report of a multicenter randomized trial. J Clin Oncol. 2002;20(3):817-825. doi:10.1200/JCO.2002.20.3.817 - DOI - PubMed
-
- Dutch Snapshot Research Group . Benchmarking recent national practice in rectal cancer treatment with landmark randomized controlled trials. Colorectal Dis. 2017;19(6):O219-O231. - PubMed
-
- Gietelink L, Wouters MW, Tanis PJ, et al. ; Dutch Surgical Colorectal Cancer Audit Group . Reduced circumferential resection margin involvement in rectal cancer surgery: results of the Dutch Surgical Colorectal Audit. J Natl Compr Canc Netw. 2015;13(9):1111-1119. doi:10.6004/jnccn.2015.0136 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
