

Temporal Risk of Nonfatal Cardiovascular Events After Chronic Obstructive Pulmonary Disease Exacerbation: A Population-based Study
- PMID: 38127850
- PMCID: PMC11531205
- DOI: 10.1164/rccm.202307-1122OC
Temporal Risk of Nonfatal Cardiovascular Events After Chronic Obstructive Pulmonary Disease Exacerbation: A Population-based Study
Abstract
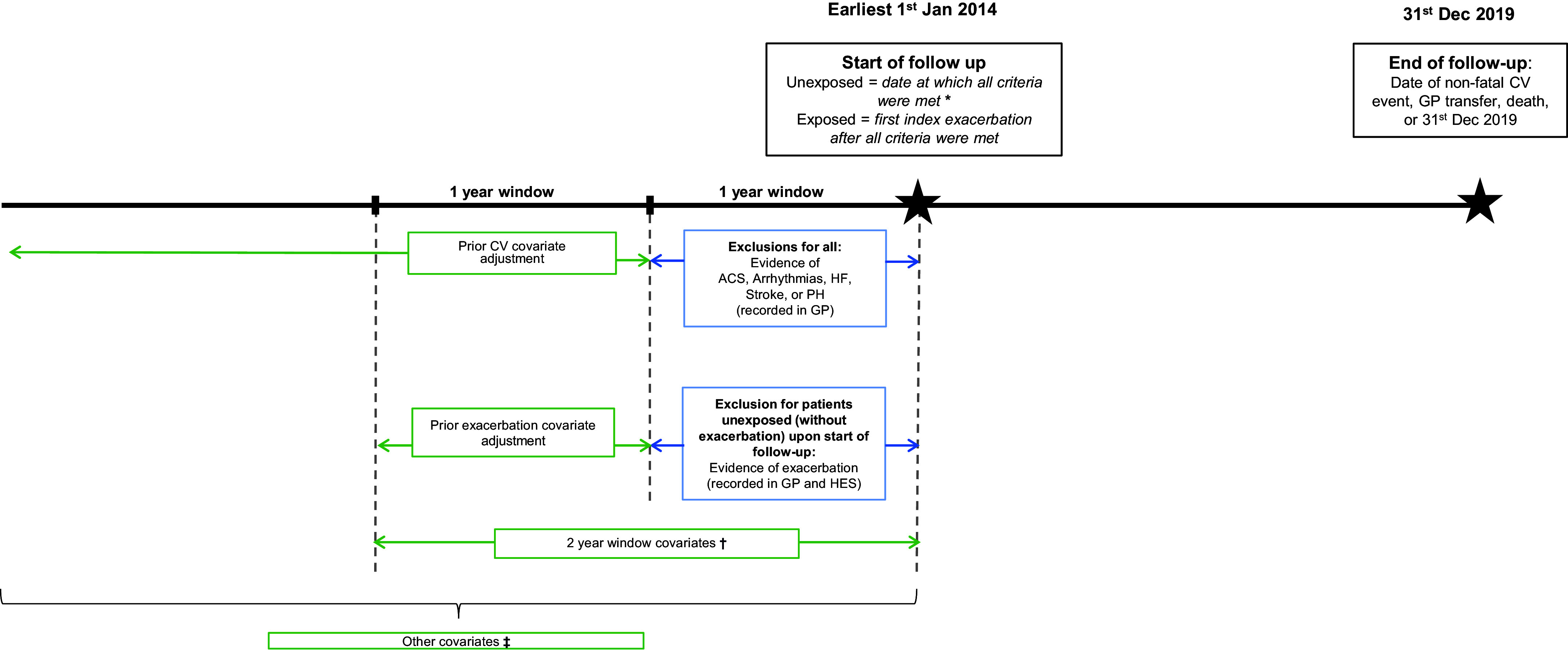
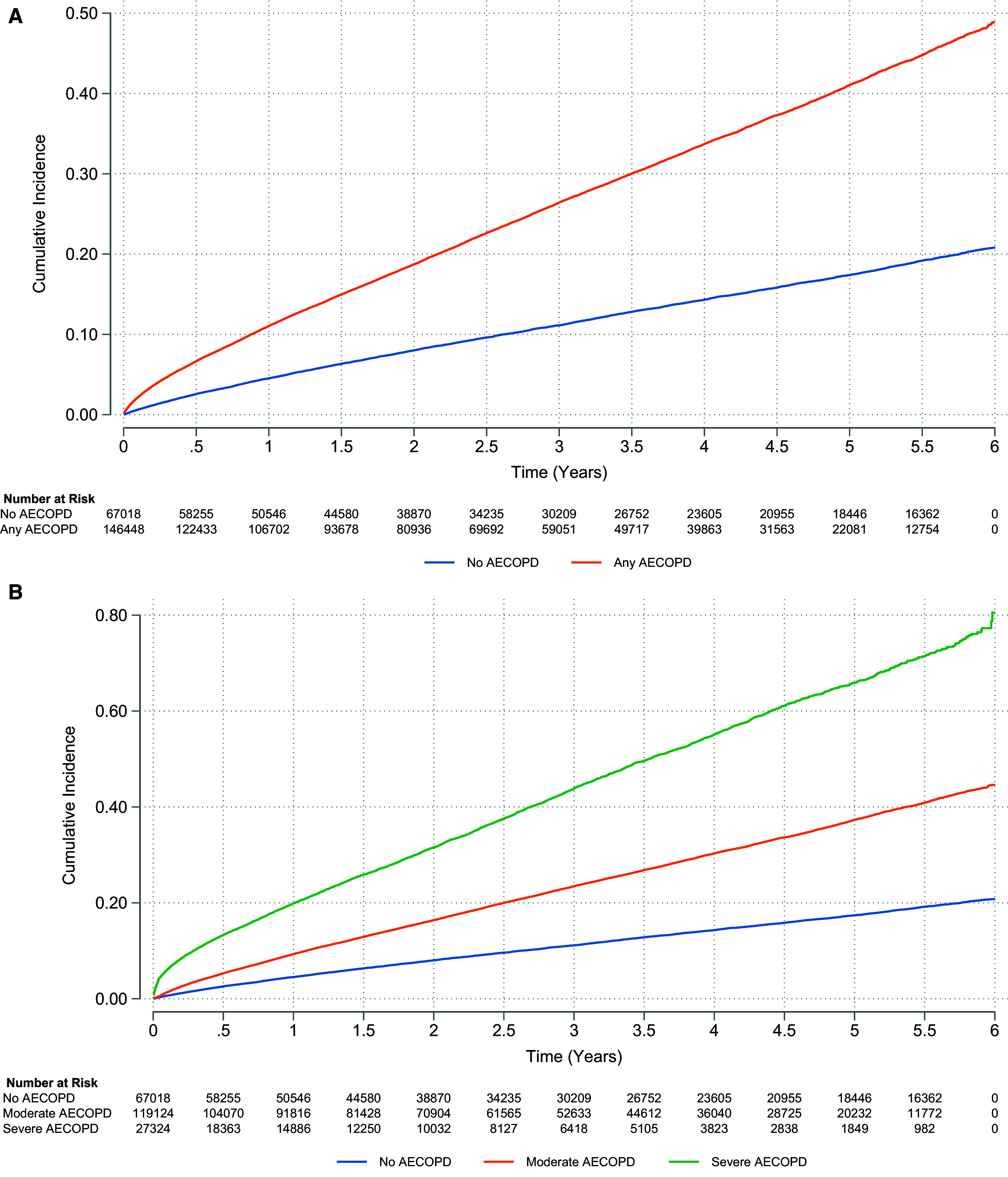
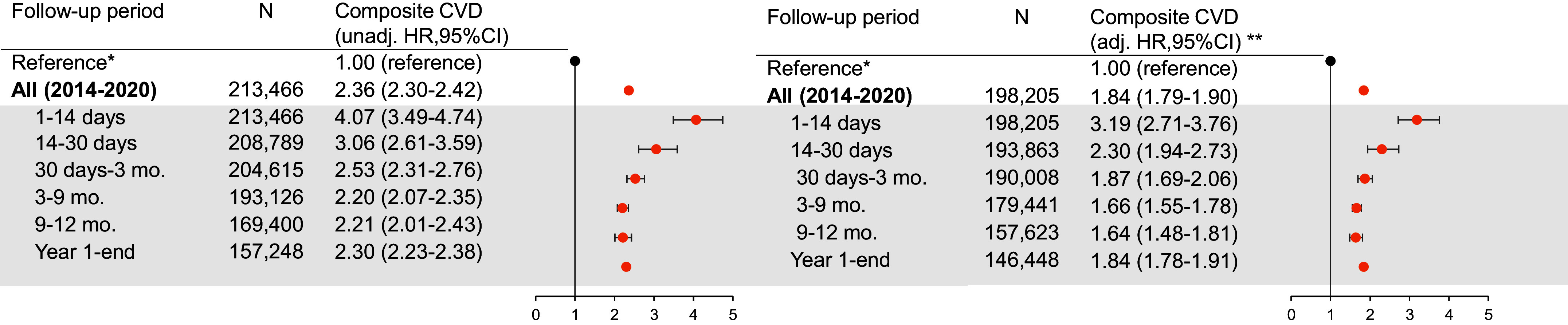
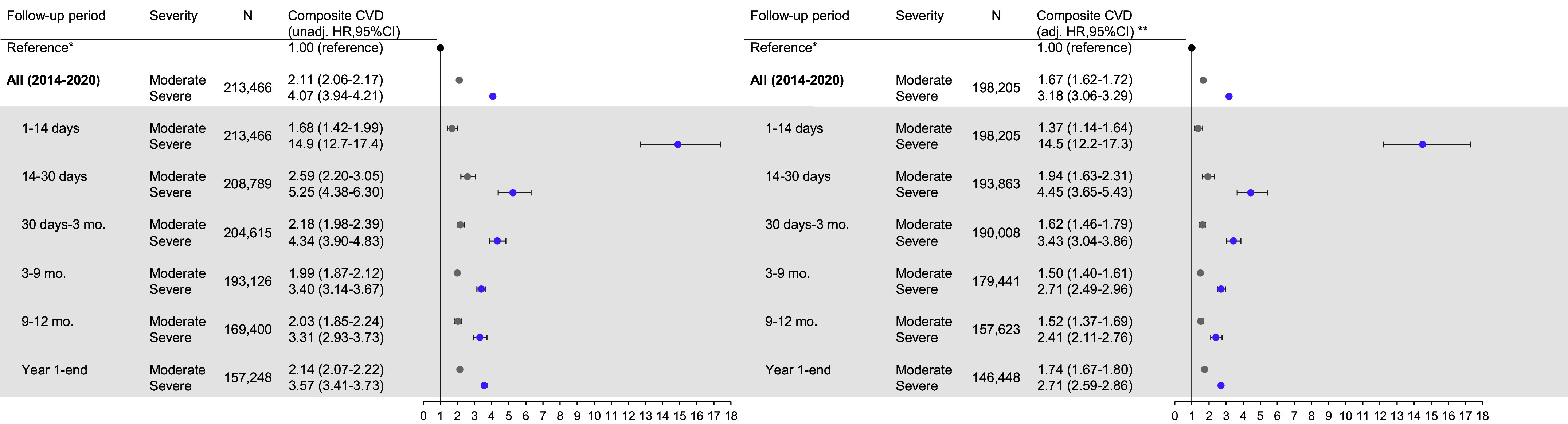
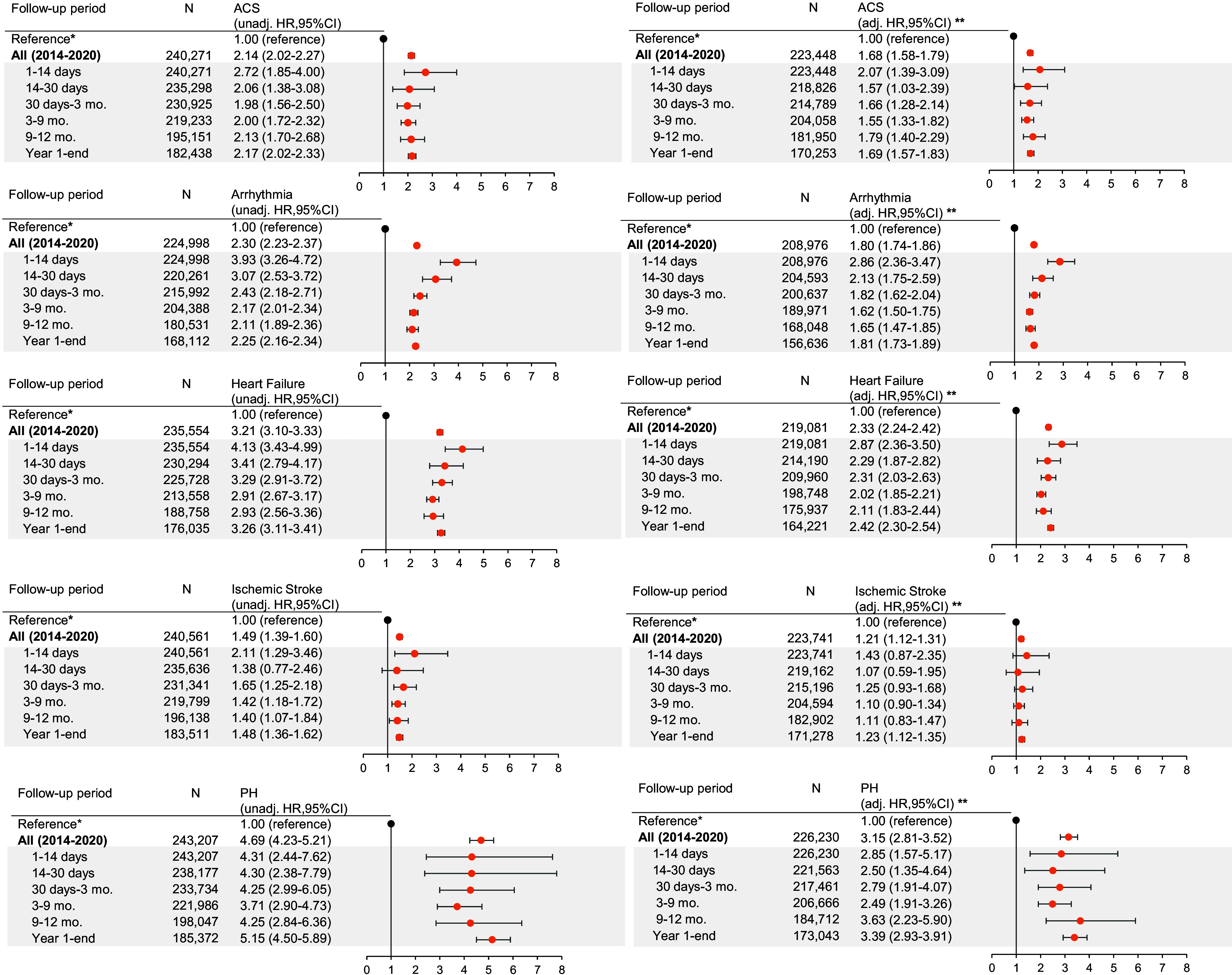
Rationale: Cardiovascular events after chronic obstructive pulmonary disease (COPD) exacerbations are recognized. Studies to date have been post hoc analyses of trials, did not differentiate exacerbation severity, included death in the cardiovascular outcome, or had insufficient power to explore individual outcomes temporally.Objectives: We explore temporal relationships between moderate and severe exacerbations and incident, nonfatal hospitalized cardiovascular events in a primary care-derived COPD cohort.Methods: We included people with COPD in England from 2014 to 2020, from the Clinical Practice Research Datalink Aurum primary care database. The index date was the date of first COPD exacerbation or, for those without exacerbations, date upon eligibility. We determined composite and individual cardiovascular events (acute coronary syndrome, arrhythmia, heart failure, ischemic stroke, and pulmonary hypertension) from linked hospital data. Adjusted Cox regression models were used to estimate average and time-stratified adjusted hazard ratios (aHRs).Measurements and Main Results: Among 213,466 patients, 146,448 (68.6%) had any exacerbation; 119,124 (55.8%) had moderate exacerbations, and 27,324 (12.8%) had severe exacerbations. A total of 40,773 cardiovascular events were recorded. There was an immediate period of cardiovascular relative rate after any exacerbation (1-14 d; aHR, 3.19 [95% confidence interval (CI), 2.71-3.76]), followed by progressively declining yet maintained effects, elevated after one year (aHR, 1.84 [95% CI, 1.78-1.91]). Hazard ratios were highest 1-14 days after severe exacerbations (aHR, 14.5 [95% CI, 12.2-17.3]) but highest 14-30 days after moderate exacerbations (aHR, 1.94 [95% CI, 1.63-2.31]). Cardiovascular outcomes with the greatest two-week effects after a severe exacerbation were arrhythmia (aHR, 12.7 [95% CI, 10.3-15.7]) and heart failure (aHR, 8.31 [95% CI, 6.79-10.2]).Conclusions: Cardiovascular events after moderate COPD exacerbations occur slightly later than after severe exacerbations; heightened relative rates remain beyond one year irrespective of severity. The period immediately after an exacerbation presents a critical opportunity for clinical intervention and treatment optimization to prevent future cardiovascular events.
Keywords: COPD; cardiovascular disease; electronic health records; epidemiology.
Figures
Comment in
-
Risk and Prevention of Cardiovacular Events after Exacerbations of Respiratory Symptoms in Patients with COPD.Am J Respir Crit Care Med. 2024 Apr 15;209(8):901-902. doi: 10.1164/rccm.202401-0040ED. Am J Respir Crit Care Med. 2024. PMID: 38319130 Free PMC article. No abstract available.
References
-
- Balbirsingh V, Mohammed AS, Turner AM, Newnham M. Cardiovascular disease in chronic obstructive pulmonary disease: a narrative review. Thorax . 2022;77:939–945. - PubMed
-
- Müllerova H, Agusti A, Erqou S, Mapel DW. Cardiovascular comorbidity in COPD: systematic literature review. Chest . 2013;144:1163–1178. - PubMed
-
- Morgan AD, Rothnie KJ, Bhaskaran K, Smeeth L, Quint JK. Chronic obstructive pulmonary disease and the risk of 12 cardiovascular diseases: a population-based study using UK primary care data. Thorax . 2018;73:877–879. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
