

Abdominal volume index, waist-to-height ratio, and waist circumference are optimal predictors of cardiometabolic abnormalities in a sample of Lebanese adults: A cross-sectional study
- PMID: 38127883
- PMCID: PMC10734963
- DOI: 10.1371/journal.pgph.0002726
Abdominal volume index, waist-to-height ratio, and waist circumference are optimal predictors of cardiometabolic abnormalities in a sample of Lebanese adults: A cross-sectional study
Abstract
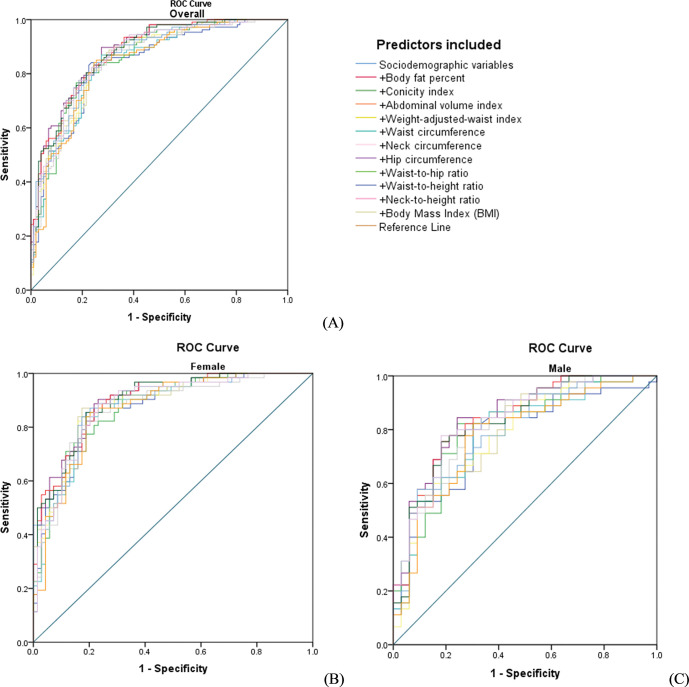
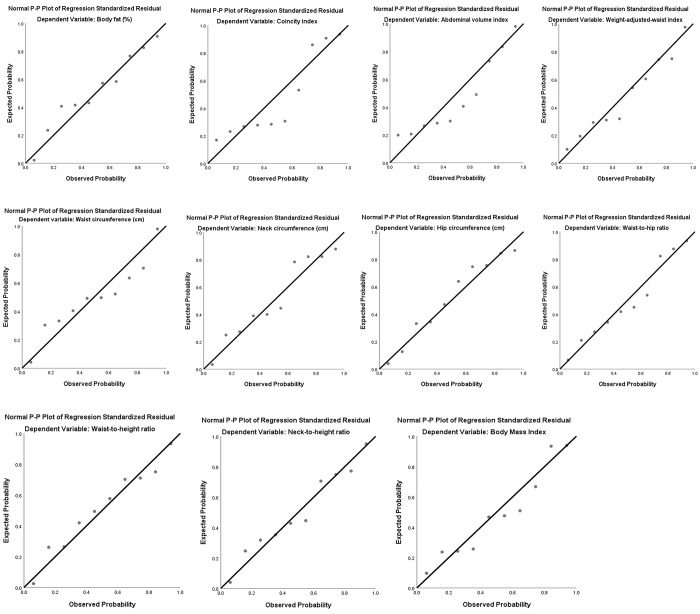
The prevalence of cardiometabolic abnormalities is high globally. This is concerning since these abnormalities increase the risk of morbidity and mortality. Using noninvasive, low-cost, and ethnic-specific anthropometric indices is crucial for widespread screening and early detection of cardiometabolic abnormalities. In this cross-sectional study, we enrolled 221 Lebanese participants (62.9% females; mean age: 43.36 ± 16.05 years; mean body mass index (BMI): 28.43 ± 6.10 Kg/m2). The main outcome measure was cardiometabolic abnormality (CMA), defined as the presence of at least two or more non-anthropometric components of the Metabolic Syndrome. Several anthropometric indices: Total body fat percent, Conicity index, Abdominal volume index (AVI), Weight-adjusted-waist index, Waist circumference (WC), Neck circumference, Hip circumference, Waist-to-hip ratio, Waist-to-height ratio (WtHR), Neck-to-height ratio, and BMI were assessed in their prediction of CMA, using logistic regression modelling and c-statistic [95% confidence intervals (CIs)], and calibration plots, as well sensitivity, specificity, and negative and positive predictive values measures. The Benjamini-Hochberg correction procedure was used to correct for multiple testing. The prevalence of CMA was 52.0% (47.5% in females and 59.8% in males). Significant associations were found between all the anthropometric indices and CMA, except for neck-to-height ratio. AVI and WC were most predictive for CMA in the total sample. WtHR and WC were most predictive in females with suggested cut-off values of 0.58 and 91.25 cm, whereas AVI and WC were most predictive in males with suggested cut-off values of 19.61 and 101.50 cm. The neck-to-height measurement had the lowest predictive ability for CMA. Adding anthropometric indices to sociodemographic variables did not significantly improve model discrimination. AVI, WHtR, and WC best predicted CMA in a sample of Lebanese adults. These less invasive, low-cost, easy-to-measure indices can be used to screen widely for CMA to better manage and prevent disease and subsequent morbidity and mortality.
Copyright: © 2023 Abboud et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644 - DOI - PubMed
-
- O’Neill S O’Driscoll L. Metabolic syndrome: a closer look at the growing epidemic and its associated pathologies. Obesity Reviews. 2015;16(1):1–12. - PubMed
-
- Bahijri SM, Al Raddadi RM, Jambi H, Alaama M-NA, Ferns G. The prevalence of metabolic syndrome in an apparently healthy, normotensive and non-diabetic population in Saudi Arabia by two definitions: implications for local practice. Journal of Endocrine and Metabolic Diseases. 2013;3:18–24.
LinkOut - more resources
Full Text Sources