

Fetoscopic Endoluminal Tracheal Occlusion for Severe, Left-Sided Congenital Diaphragmatic Hernia: The North American Fetal Therapy Network Fetoscopic Endoluminal Tracheal Occlusion Consortium Experience
- PMID: 38128107
- PMCID: PMC10863657
- DOI: 10.1097/AOG.0000000000005491
Fetoscopic Endoluminal Tracheal Occlusion for Severe, Left-Sided Congenital Diaphragmatic Hernia: The North American Fetal Therapy Network Fetoscopic Endoluminal Tracheal Occlusion Consortium Experience
Abstract
Objective: To report the outcomes of fetoscopic endoluminal tracheal occlusion in a multicenter North American cohort of patients with isolated, left-sided congenital diaphragmatic hernia (CDH) and to compare neonatal mortality and morbidity in patients with severe left-sided congenital diaphragmatic hernia who underwent fetoscopic endoluminal tracheal occlusion with those expectantly managed.
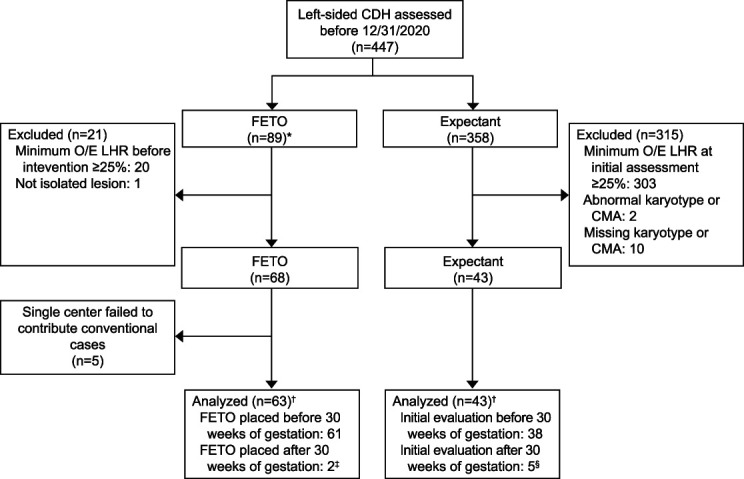
Methods: We analyzed data from 10 centers in the NAFTNet (North American Fetal Therapy Network) FETO (Fetoscopic Endoluminal Tracheal Occlusion) Consortium registry, collected between November 1, 2008, and December 31, 2020. In addition to reporting procedure-related surgical outcomes of fetoscopic endoluminal tracheal occlusion, we performed a comparative analysis of fetoscopic endoluminal tracheal occlusion compared with contemporaneous expectantly managed patients.
Results: Fetoscopic endoluminal tracheal occlusion was successfully performed in 87 of 89 patients (97.8%). Six-month survival in patients with severe left-sided congenital diaphragmatic hernia did not differ significantly between patients who underwent fetoscopic endoluminal tracheal occlusion and those managed expectantly (69.8% vs 58.1%, P =.30). Patients who underwent fetoscopic endoluminal tracheal occlusion had higher rates of preterm prelabor rupture of membranes (54.0% vs 14.3%, P <.001), earlier gestational age at delivery (median 35.0 weeks vs 38.3 weeks, P <.001), and lower birth weights (mean 2,487 g vs 2,857 g, P =.001). On subanalysis, in patients for whom all recorded observed-to-expected lung/head ratio measurements were below 25%, patients with fetoscopic endoluminal tracheal occlusion required fewer days of extracorporeal membrane oxygenation (ECMO) (median 9.0 days vs 17.0 days, P =.014).
Conclusion: In this cohort, fetoscopic endoluminal tracheal occlusion was successfully implemented across several North American fetal therapy centers. Although survival was similar among patients undergoing fetoscopic endoluminal tracheal occlusion and those expectantly managed, fetoscopic endoluminal tracheal occlusion in North American centers may reduce morbidity, as suggested by fewer days of ECMO in those patients with persistently reduced lung volumes (observed-to-expected lung/head ratio below 25%).
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Financial Disclosure Eric Bergh disclosed that the NFocus Goldvalve balloon is no longer commercially available, and he receives royalties from UpToDate. Dr. Cromblehome disclosed that the Balt GOLDBAL2 balloon and catheter and Storz fetoscope are used under an investigational device exemption from the Food and Drug Administration, which are not otherwise available for use in the United States. Ahmet A. Baschat disclosed that the instrumentation was provided in-kind by Karl Storz, and he receives royalties from UpToDate. Holly Hedrick receives royalties from UpToDate. The other authors did not report any potential conflicts of interest.
Figures
Similar articles
-
Fetoscopic endoluminal tracheal occlusion vs expectant management for fetuses with severe left-sided congenital diaphragmatic hernia.Am J Obstet Gynecol MFM. 2024 Feb;6(2):101248. doi: 10.1016/j.ajogmf.2023.101248. Epub 2023 Dec 8. Am J Obstet Gynecol MFM. 2024. PMID: 38070678
-
The randomized Tracheal Occlusion To Accelerate Lung growth (TOTAL)-trials on fetal surgery for congenital diaphragmatic hernia: reanalysis using pooled data.Am J Obstet Gynecol. 2022 Apr;226(4):560.e1-560.e24. doi: 10.1016/j.ajog.2021.11.1351. Epub 2021 Nov 19. Am J Obstet Gynecol. 2022. PMID: 34808130 Clinical Trial.
-
Survival outcome in severe left-sided congenital diaphragmatic hernia with and without fetal endoscopic tracheal occlusion in a country with suboptimal neonatal management.Ultrasound Obstet Gynecol. 2020 Oct;56(4):516-521. doi: 10.1002/uog.21993. Epub 2020 Aug 30. Ultrasound Obstet Gynecol. 2020. PMID: 32068928
-
Postnatal care setting and survival after fetoscopic tracheal occlusion for severe congenital diaphragmatic hernia: A systematic review and meta-analysis.J Pediatr Surg. 2022 Dec;57(12):819-825. doi: 10.1016/j.jpedsurg.2022.05.011. Epub 2022 May 19. J Pediatr Surg. 2022. PMID: 35680463
-
Fetal endoscopic tracheal occlusion for moderate and severe congenital diaphragmatic hernia: a systematic review and meta-analysis of randomized controlled trials.Pediatr Surg Int. 2022 Sep;38(9):1217-1226. doi: 10.1007/s00383-022-05170-7. Epub 2022 Jul 15. Pediatr Surg Int. 2022. PMID: 35838786
Cited by
-
Management advances for congenital diaphragmatic hernia: integrating prenatal and postnatal perspectives.Transl Pediatr. 2024 Apr 30;13(4):643-662. doi: 10.21037/tp-23-602. Epub 2024 Apr 18. Transl Pediatr. 2024. PMID: 38715680 Free PMC article. Review.
-
Prenatal Surgery for Open Fetal Spina Bifida in Patients with Obesity: A Review of Current Evidence and Future Directions.J Clin Med. 2024 Sep 24;13(19):5661. doi: 10.3390/jcm13195661. J Clin Med. 2024. PMID: 39407721 Free PMC article. Review.
-
Fetoscopic Tracheal Occlusion for Isolated Severe Left Diaphragmatic Hernia: A Systematic Review and Meta-Analysis.J Clin Med. 2024 Jun 18;13(12):3572. doi: 10.3390/jcm13123572. J Clin Med. 2024. PMID: 38930102 Free PMC article. Review.
-
Fetal Endoscopic Tracheal Occlusion (FETO) for Left and Right Congenital Diaphragmatic Hernia in Canada.Prenat Diagn. 2025 Jun;45(6):778-786. doi: 10.1002/pd.6803. Epub 2025 Apr 29. Prenat Diagn. 2025. PMID: 40302114 Free PMC article.
-
Clinical outcomes after implementation of a physiologic pre-operative management strategy in neonates with congenital diaphragmatic hernia.J Perinatol. 2025 Jul 18. doi: 10.1038/s41372-025-02362-6. Online ahead of print. J Perinatol. 2025. PMID: 40676197
References
-
- Harrison MR, Mychaliska GB, Albanese CT, Jennings RW, Farrell JA, Hawgood S, et al. Correction of congenital diaphragmatic hernia in utero, IX: fetuses with poor prognosis (liver herniation and low lung-to-head ratio) can be saved by fetoscopic temporary tracheal occlusion. J Pediatr Surg 1998;33:1017–22. doi: 10.1016/s0022-3468(98)90524-3 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
