

Safety and immunogenicity of a synthetic nanoparticle-based, T cell priming peptide vaccine against dengue in healthy adults in Switzerland: a double-blind, randomized, vehicle-controlled, phase 1 study
- PMID: 38128414
- PMCID: PMC10776924
- DOI: 10.1016/j.ebiom.2023.104922
Safety and immunogenicity of a synthetic nanoparticle-based, T cell priming peptide vaccine against dengue in healthy adults in Switzerland: a double-blind, randomized, vehicle-controlled, phase 1 study
Abstract
Background: Vaccines that minimize the risk of vaccine-induced antibody-dependent enhancement and severe dengue are needed to address the global health threat posed by dengue. This study assessed the safety and immunogenicity of a gold nanoparticle (GNP)-based, multi-valent, synthetic peptide dengue vaccine candidate (PepGNP-Dengue), designed to provide protective CD8+ T cell immunity, without inducing antibodies.
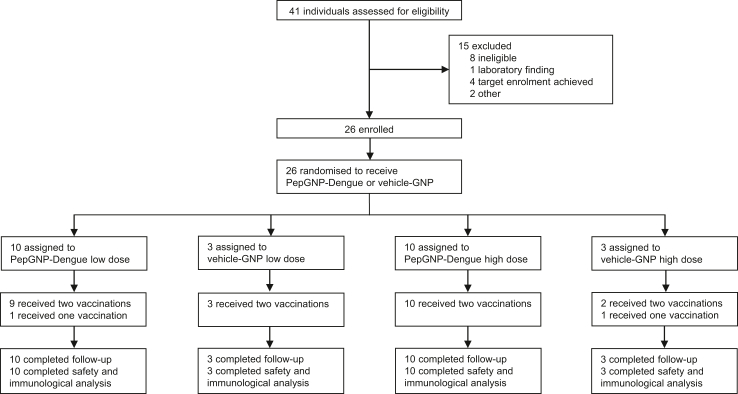
Methods: In this randomized, double-blind, vehicle-controlled, phase 1 trial (NCT04935801), healthy naïve individuals aged 18-45 years recruited at the Centre for primary care and public health, Lausanne, Switzerland, were randomly assigned to receive PepGNP-Dengue or comparator (GNP without peptides [vehicle-GNP]). Randomization was stratified into four groups (low dose [LD] and high dose [HD]), allocation was double-blind from participants and investigators. Two doses were administered by intradermal microneedle injection 21 days apart. Primary outcome was safety, secondary outcome immunogenicity. Analysis was by intention-to-treat for safety, intention-to-treat and per protocol for immunogenicity.
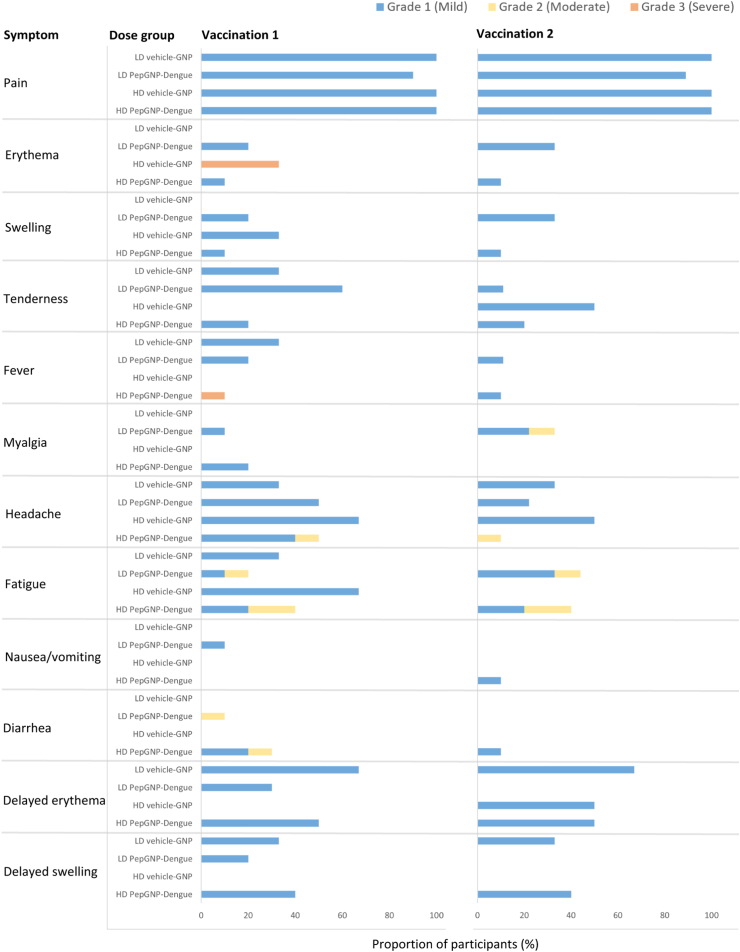
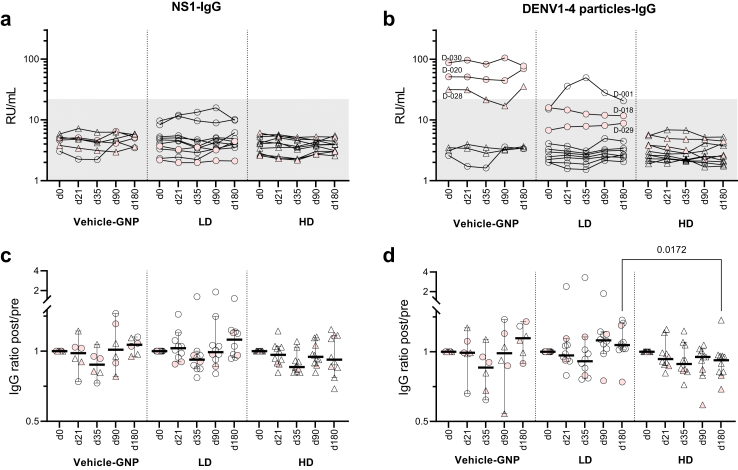
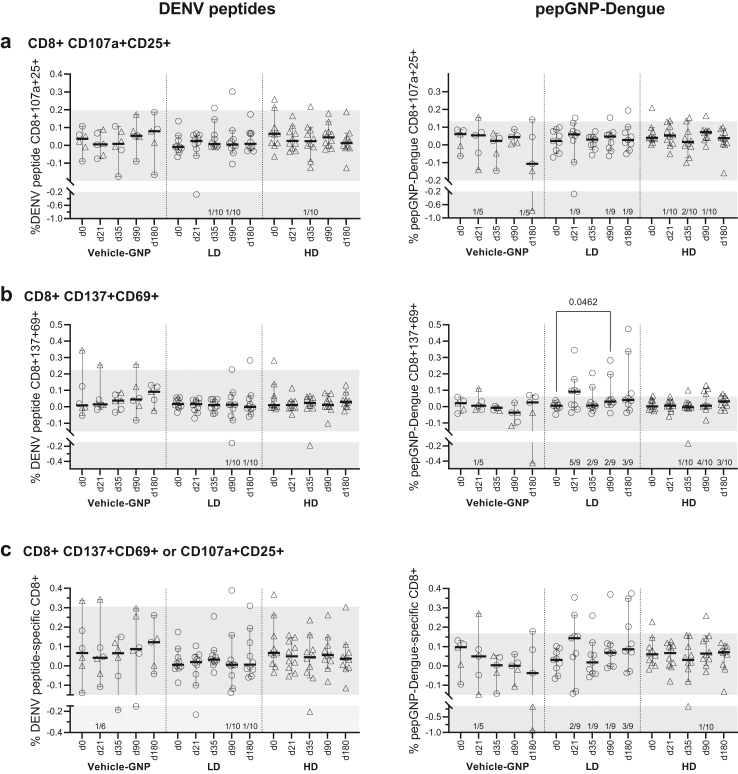
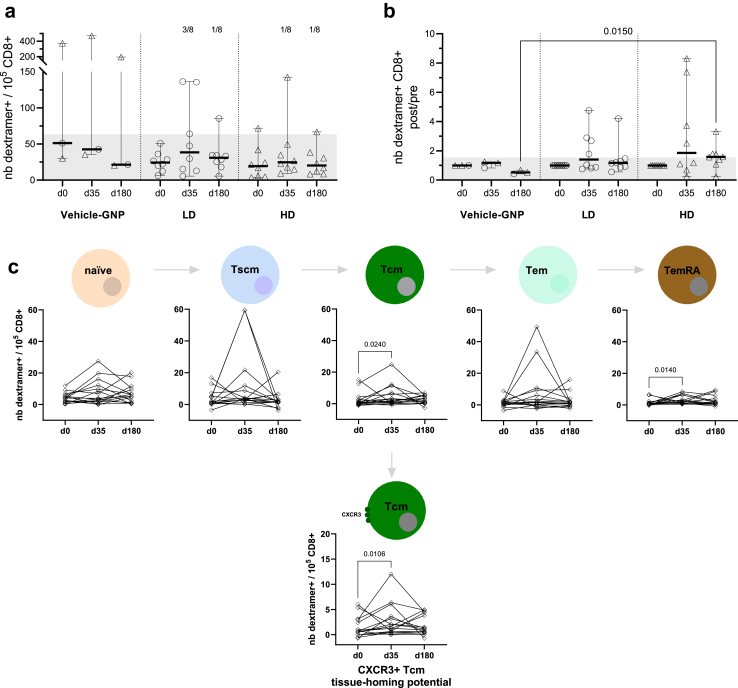
Findings: 26 participants were enrolled (August-September 2021) to receive PepGNP-Dengue (LD or HD, n = 10 each) or vehicle-GNP (LD or HD, n = 3 each). No vaccine-related serious adverse events occurred. Most (90%) related adverse events were mild; injection site pain and transient discoloration were most frequently reported. Injection site erythema occurred in 58% of participants. As expected, PepGNP-Dengue did not elicit anti-DENV antibodies of significance. Significant increases were observed in specific CD8+ T cells and dengue dextramer+ memory cell subsets in the LD PepGNP-Dengue but not in the HD PepGNP-Dengue or vehicle-GNP groups, specifically PepGNP-activated CD137+CD69+CD8+ T cells (day 90, +0.0318%, 95% CI: 0.0088-0.1723, p = 0.046), differentiated effector memory (TemRA) and central memory (Tcm) CD8+ T cells (day 35, +0.8/105 CD8+, 95% CI: 0.19-5.13, p = 0.014 and +1.34/105 CD8+, 95% CI: 0.1-7.34, p = 0.024, respectively).
Interpretation: Results provide proof of concept that a synthetic nanoparticle-based peptide vaccine can successfully induce virus-specific CD8+ T cells. The favourable safety profile and cellular responses observed support further development of PepGNP-Dengue.
Funding: Emergex Vaccines Holding Limited.
Keywords: Dengue vaccine; Dengue virus; Nanoparticle-based vaccine; T cell immunity.
Copyright © 2023 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests All authors and the PV CRO Qvigilance declare no competing interests.
Figures
References
-
- World Health Organization . 2017. Fact sheets: dengue and severe dengue.https://apps.who.int/mediacentre/factsheets/fs117/en/index.html Available from:
-
- World Health Organization . 2019. Ten threats to Global Health in 2019.https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-... Available from:
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
