

Gut microbiota predicts severity and reveals novel metabolic signatures in acute pancreatitis
- PMID: 38129103
- PMCID: PMC10894816
- DOI: 10.1136/gutjnl-2023-330987
Gut microbiota predicts severity and reveals novel metabolic signatures in acute pancreatitis
Abstract
Objective: Early disease prediction is challenging in acute pancreatitis (AP). Here, we prospectively investigate whether the microbiome predicts severity of AP (Pancreatitis-Microbiome As Predictor of Severity; P-MAPS) early at hospital admission.
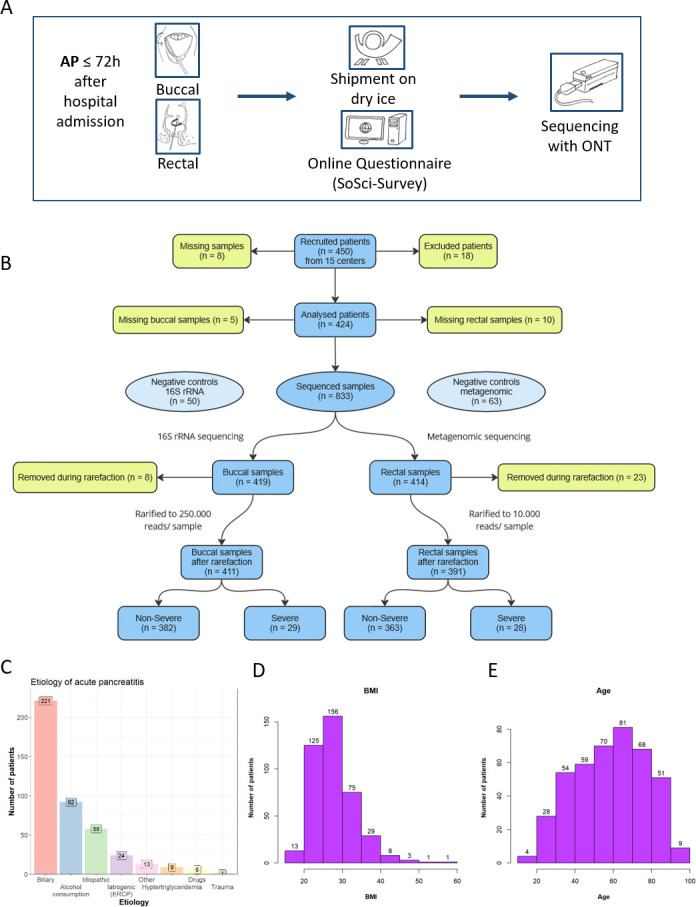
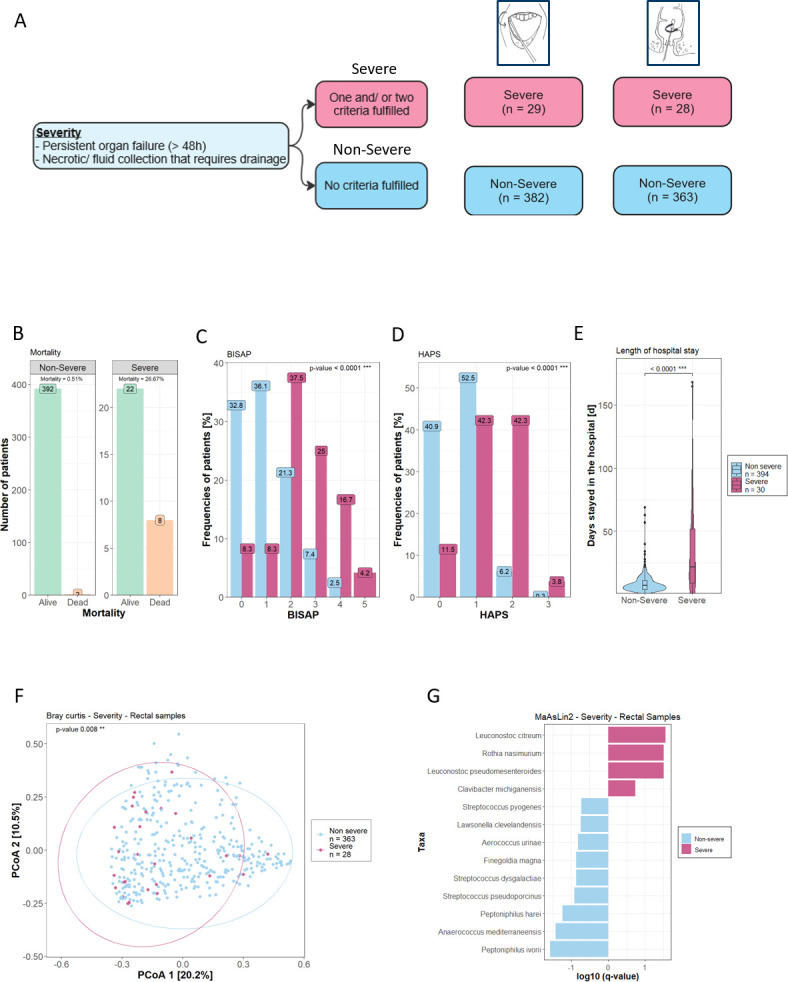
Design: Buccal and rectal microbial swabs were collected from 424 patients with AP within 72 hours of hospital admission in 15 European centres. All samples were sequenced by full-length 16S rRNA and metagenomic sequencing using Oxford Nanopore Technologies. Primary endpoint was the association of the orointestinal microbiome with the revised Atlanta classification (RAC). Secondary endpoints were mortality, length of hospital stay and severity (organ failure >48 hours and/or occurrence of pancreatic collections requiring intervention) as post hoc analysis. Multivariate analysis was conducted from normalised microbial and corresponding clinical data to build classifiers for predicting severity. For functional profiling, gene set enrichment analysis (GSEA) was performed and normalised enrichment scores calculated.
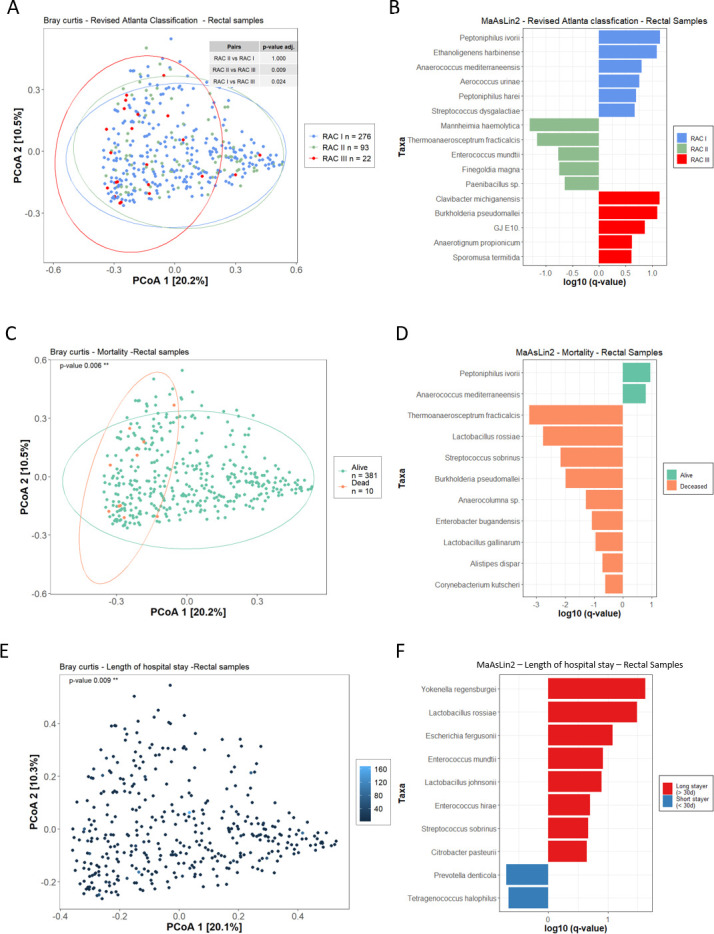
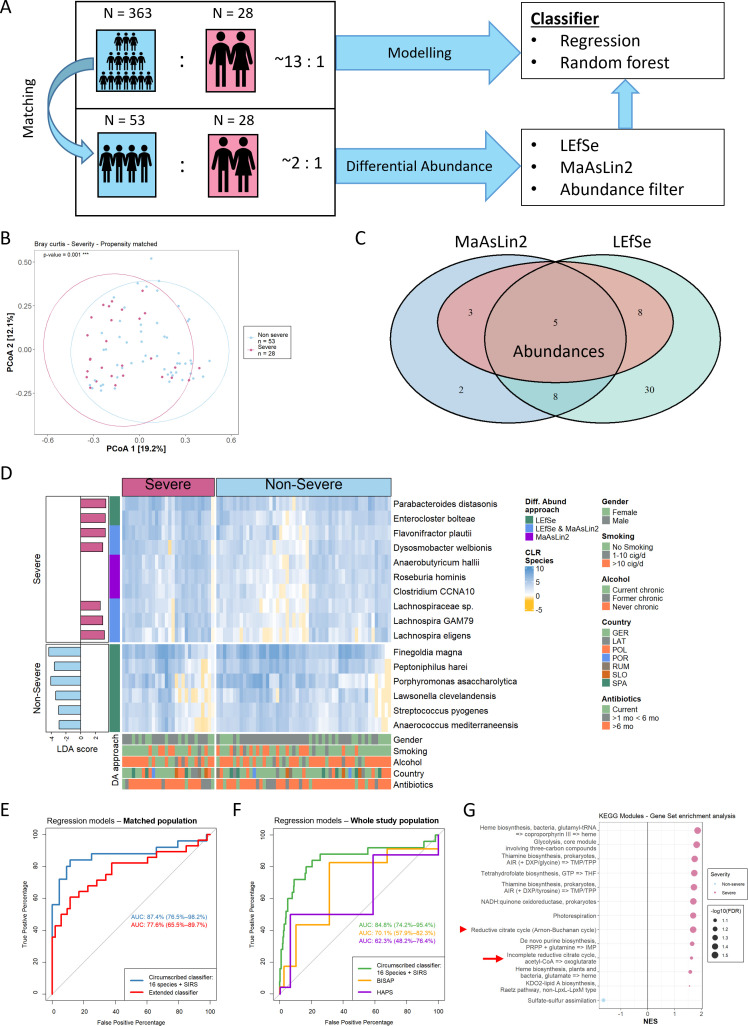
Results: After data processing, 411 buccal and 391 rectal samples were analysed. The intestinal microbiome significantly differed for the RAC (Bray-Curtis, p value=0.009), mortality (Bray-Curtis, p value 0.006), length of hospital stay (Bray-Curtis, p=0.009) and severity (Bray-Curtis, p value=0.008). A classifier for severity with 16 different species and systemic inflammatory response syndrome achieved an area under the receiving operating characteristic (AUROC) of 85%, a positive predictive value of 67% and a negative predictive value of 94% outperforming established severity scores. GSEA revealed functional pathway units suggesting elevated short-chain fatty acid (SCFA) production in severe AP.
Conclusions: The orointestinal microbiome predicts clinical hallmark features of AP, and SCFAs may be used for future diagnostic and therapeutic concepts.
Trial registration number: NCT04777812.
Keywords: acute pancreatitis; pancreas; pancreatic disorders.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous