

Low-load blood flow restriction strength training in patients with COPD: a randomised single-blind pilot study
- PMID: 38129116
- PMCID: PMC10958309
- DOI: 10.1136/thorax-2023-220546
Low-load blood flow restriction strength training in patients with COPD: a randomised single-blind pilot study
Abstract
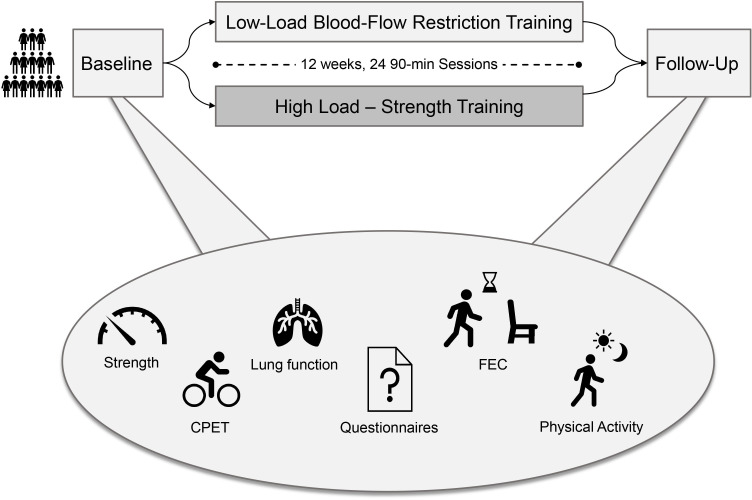
Objective: The objective of this study is to compare the effectiveness of lower limb low-load blood flow restriction training (LL-BFRT) with high-load strength training (HL-ST) as part of an outpatient pulmonary rehabilitation programme on leg strength in patients with chronic obstructive pulmonary disease (COPD).
Methods: Participants were randomised to LL-BFRT or HL-ST (24 sessions). LL-BFRT was done at 30% 1-repetition maximum (1-RM) with 70% arterial occlusion pressure. HL-ST was done at 70% 1-RM. Primary outcome was isometric strength of knee extensors and flexors. Secondary outcomes were 1-RM, functional exercise capacity, physical activity, symptom burden and health-related quality of life. Perceptions of dyspnoea and leg fatigue were recorded after every exercise. We compared groups with t-tests.
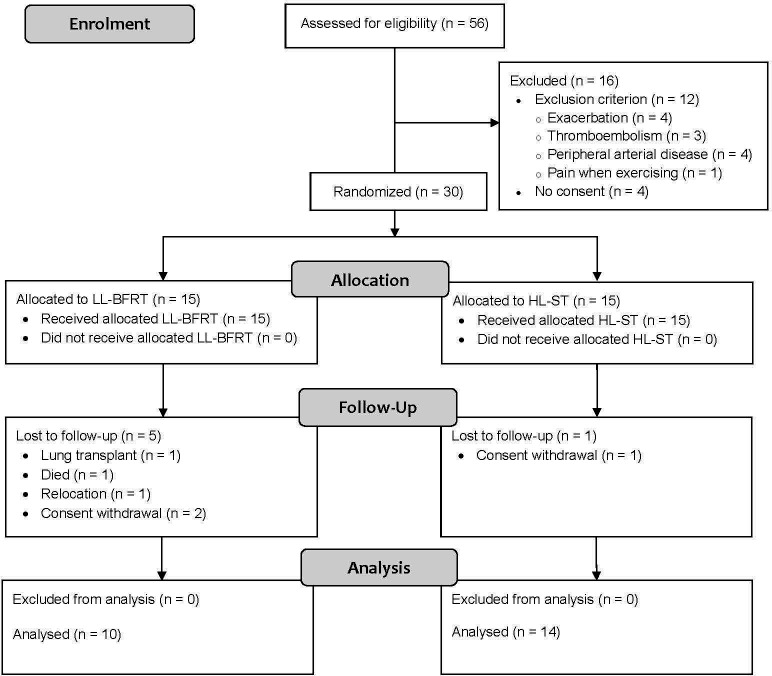
Results: We included 30 participants (13 women, 17 men, 64 (9) years, forced expiratory volume in 1 s 47 (18)% pred.), 24 completed the study. Isometric knee extensor strength improved to a clinically relevant degree in both legs in both groups (LL-BFRT: right leg 9 (20) Nm, left leg 10 (18) Nm; HL-ST: right leg 15 (26) Nm, left leg 16 (30) Nm, data are mean (SD)), without statistically significant or clinically relevant between-group differences (right leg mean difference= -6.4, 95% CI= -13.20 to 25.92 Nm, left leg mean difference= -5.6, 95% CI= -15.44 to 26.55 Nm). 1 min sit-to-stand test performance improved to a clinically relevant degree only in the LL-BFRT group (4 (4) vs 1 (5) repetitions). Interestingly, physical activity improved to a clinically relevant degree only in the LL-BFRT group (1506 (2441) vs -182 (1971) steps/day). LL-BFRT lowered perceived in-exercise dyspnoea and increased leg fatigue compared with HL-ST in the initial 12 trainings.
Conclusion: In patients with stable COPD undergoing outpatient pulmonary rehabilitation, LL-BFRT was not superior to HL-ST in improving leg strength. LL-BFRT led to similar strength gains as HL-ST while reducing perceptions of dyspnoea in the initial training phase.
Trial registration number: NCT04151771.
Keywords: exercise; pulmonary rehabilitation.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DK, MK, AM, CA, MP, NG and NAS have nothing to disclose. CC reports personal fees from Roche, personal fees from Novartis, personal fees from Boehringer, personal fees from GSK, personal fees from Astra Zeneca, personal fees from Sanofi, personal fees from Vifor, personal fees from Mundipharma, personal fees from Daiichi Synkyo, personal fees from CSL Behring, all outside the submitted work.
Figures


References
-
- Global Initiative for Chronic Obstructive Lung Disease . Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2023 report). 2023.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical