

Prognostic utility and characterization of left ventricular hypertrophy using global thickness
- PMID: 38129418
- PMCID: PMC10740032
- DOI: 10.1038/s41598-023-48173-7
Prognostic utility and characterization of left ventricular hypertrophy using global thickness
Abstract
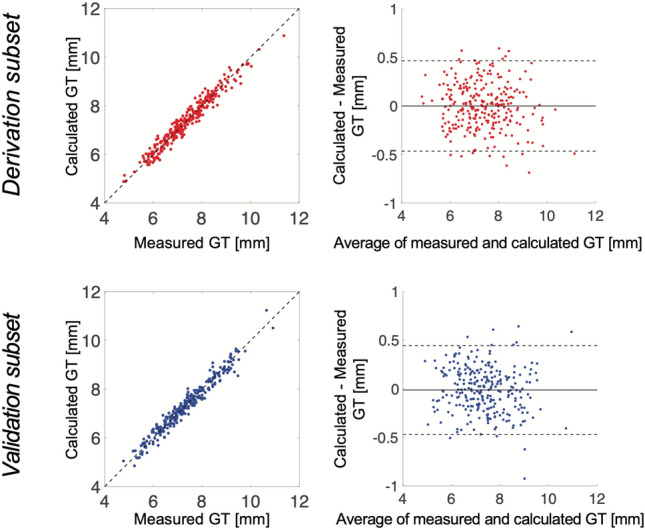
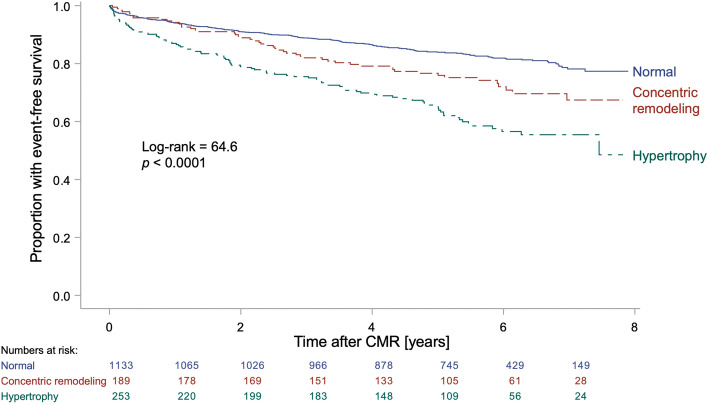
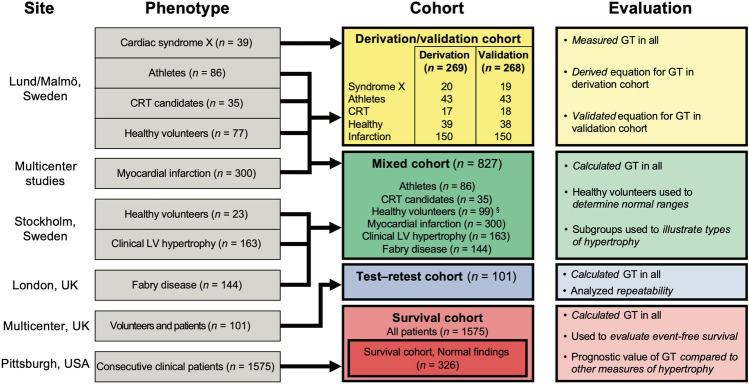
Cardiovascular magnetic resonance (CMR) can accurately measure left ventricular (LV) mass, and several measures related to LV wall thickness exist. We hypothesized that prognosis can be used to select an optimal measure of wall thickness for characterizing LV hypertrophy. Subjects having undergone CMR were studied (cardiac patients, n = 2543; healthy volunteers, n = 100). A new measure, global wall thickness (GT, GTI if indexed to body surface area) was accurately calculated from LV mass and end-diastolic volume. Among patients with follow-up (n = 1575, median follow-up 5.4 years), the most predictive measure of death or hospitalization for heart failure was LV mass index (LVMI) (hazard ratio (HR)[95% confidence interval] 1.16[1.12-1.20], p < 0.001), followed by GTI (HR 1.14[1.09-1.19], p < 0.001). Among patients with normal findings (n = 326, median follow-up 5.8 years), the most predictive measure was GT (HR 1.62[1.35-1.94], p < 0.001). GT and LVMI could characterize patients as having a normal LV mass and wall thickness, concentric remodeling, concentric hypertrophy, or eccentric hypertrophy, and the three abnormal groups had worse prognosis than the normal group (p < 0.05 for all). LV mass is highly prognostic when mass is elevated, but GT is easily and accurately calculated, and adds value and discrimination amongst those with normal LV mass (early disease).
© 2023. The Author(s).
Conflict of interest statement
ML, JN, RT, EM, KC, AS, PS, and MU are affiliated with Karolinska University Hospital which has a research agreement with Siemens regarding cardiovascular magnetic resonance imaging. EH is the founder of Medviso AB (Lund, Sweden), manufacturer of medical image analysis software. MC and HE have received consultancy fees from Imacor AB (Lund, Sweden) for cardiac MRI analysis. RB has been a speaker consultant for Medtronic (Dublin, Ireland) and for Abbott (Lake Bluff, Illinois, USA), and is on the advisory board for Pfizer (New York, New York, USA). JN has been a speaker for Orion Pharma (Esbo, Finland). HA is a stockholder in Imacor AB (Lund, Sweden). The remaining authors declare no competing interests.
Figures



References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
