

Etiology of Acute Lower Respiratory Illness Hospitalizations Among Infants in 4 Countries
- PMID: 38130597
- PMCID: PMC10733183
- DOI: 10.1093/ofid/ofad580
Etiology of Acute Lower Respiratory Illness Hospitalizations Among Infants in 4 Countries
Abstract
Background: Recent studies explored which pathogens drive the global burden of pneumonia hospitalizations among young children. However, the etiology of broader acute lower respiratory tract infections (ALRIs) remains unclear.
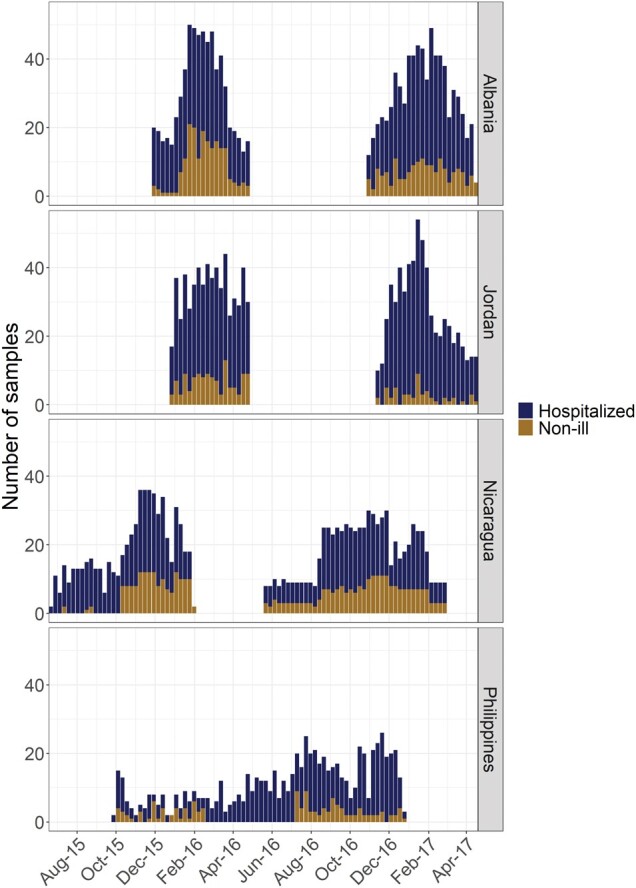
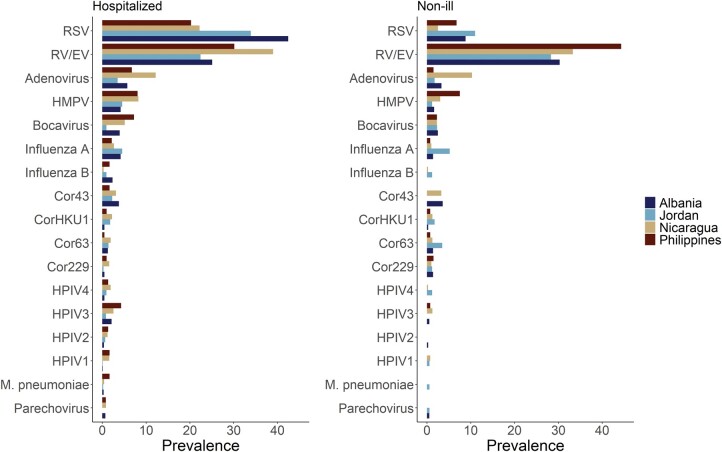
Methods: Using a multicountry study (Albania, Jordan, Nicaragua, and the Philippines) of hospitalized infants and non-ill community controls between 2015 and 2017, we assessed the prevalence and severity of viral infections and coinfections. We also estimated the proportion of ALRI hospitalizations caused by 21 respiratory pathogens identified via multiplex real-time reverse transcription polymerase chain reaction with bayesian nested partially latent class models.
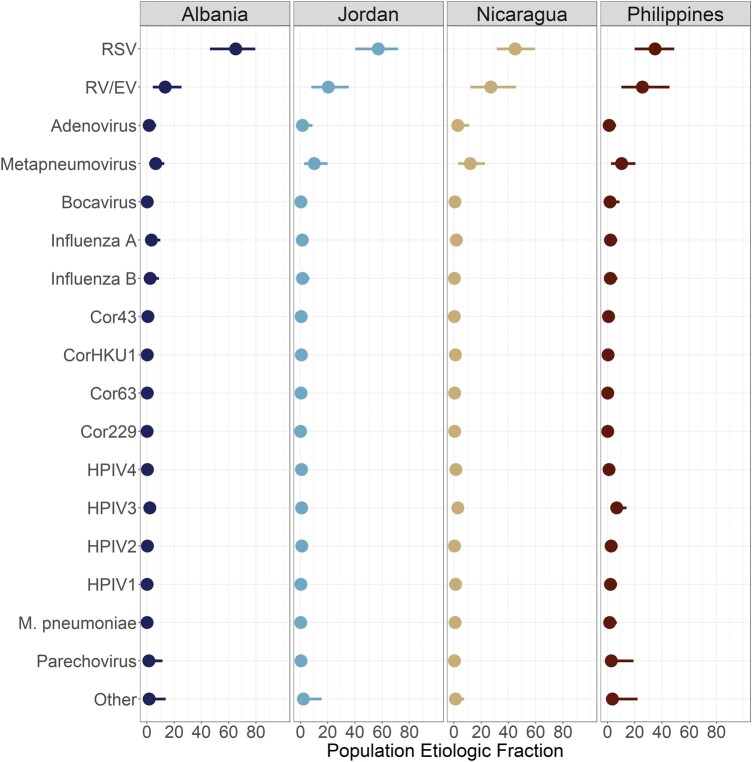
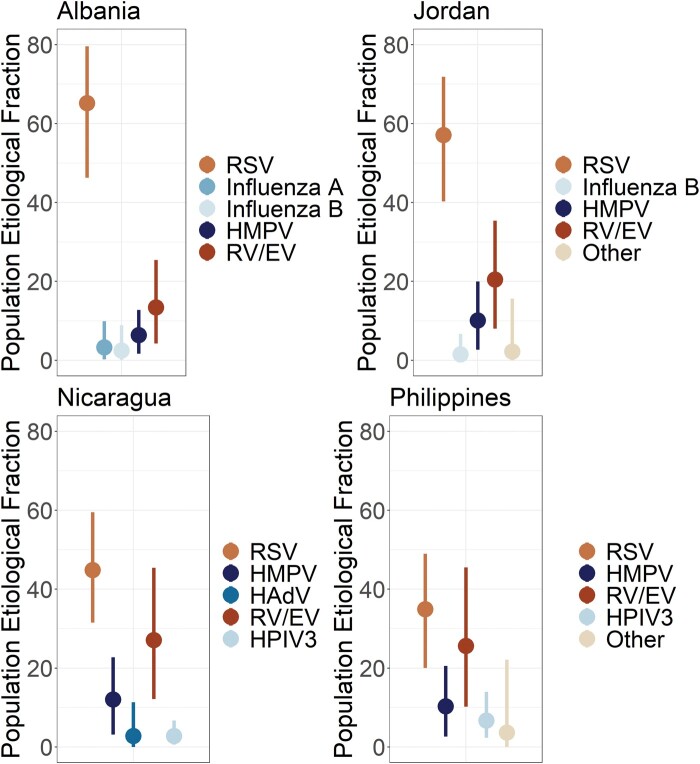
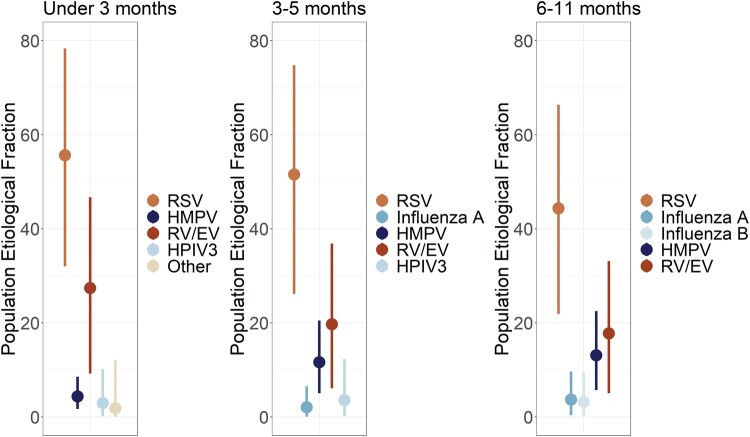
Results: An overall 3632 hospitalized infants and 1068 non-ill community controls participated in the study and had specimens tested. Among hospitalized infants, 1743 (48.0%) met the ALRI case definition for the etiology analysis. After accounting for the prevalence in non-ill controls, respiratory syncytial virus (RSV) was responsible for the largest proportion of ALRI hospitalizations, although the magnitude varied across sites-ranging from 65.2% (95% credible interval, 46.3%-79.6%) in Albania to 34.9% (95% credible interval, 20.0%-49.0%) in the Philippines. While the fraction of ALRI hospitalizations caused by RSV decreased as age increased, it remained the greatest driver. After RSV, rhinovirus/enterovirus (range, 13.4%-27.1%) and human metapneumovirus (range, 6.3%-12.0%) were the next-highest contributors to ALRI hospitalizations.
Conclusions: We observed substantial numbers of ALRI hospitalizations, with RSV as the largest source, particularly in infants aged <3 months. This underscores the potential for vaccines and long-lasting monoclonal antibodies on the horizon to reduce the burden of ALRI in infants worldwide.
Keywords: RSV; etiology; global health; influenza virus; respiratory infections.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. A. G. serves on a scientific advisory board for Janssen. E. A. F. S. reports grants and consulting fees to the institution from Merck & Co and Pfizer Inc; grants to the institution from Astra Zeneca Inc, Roche Pharmaceuticals, and Johnson & Johnson; consulting fees to the institution from Sanofi Pasteur, Cidara Therapeutics, Adiago Therapeutics, and Nuance Pharmaceuticals; manuscript writing support from Pfizer Inc and Astra Zeneca Inc; support for attending a meeting Astra Zeneca Inc; and participation on a data and safety monitoring board from AbbVie Inc, GlaxoSmithKline plc, and the Bill and Melinda Gates Foundation. None of these are directly related to this manuscript. All other authors report no potential conflicts.
Figures
References
-
- World Health Organization . Causes of child mortality. 2017. Available at: https://www.who.int/gho/child_health/mortality/causes/en/. Accessed 1 February 2023.
LinkOut - more resources
Full Text Sources
Miscellaneous
