

Paraganglioma-induced reverse takotsubo syndrome treated with extracorporeal membrane oxygenation in a young patient with a history of malignancy: a case report
- PMID: 38130863
- PMCID: PMC10733169
- DOI: 10.1093/ehjcr/ytad591
Paraganglioma-induced reverse takotsubo syndrome treated with extracorporeal membrane oxygenation in a young patient with a history of malignancy: a case report
Abstract
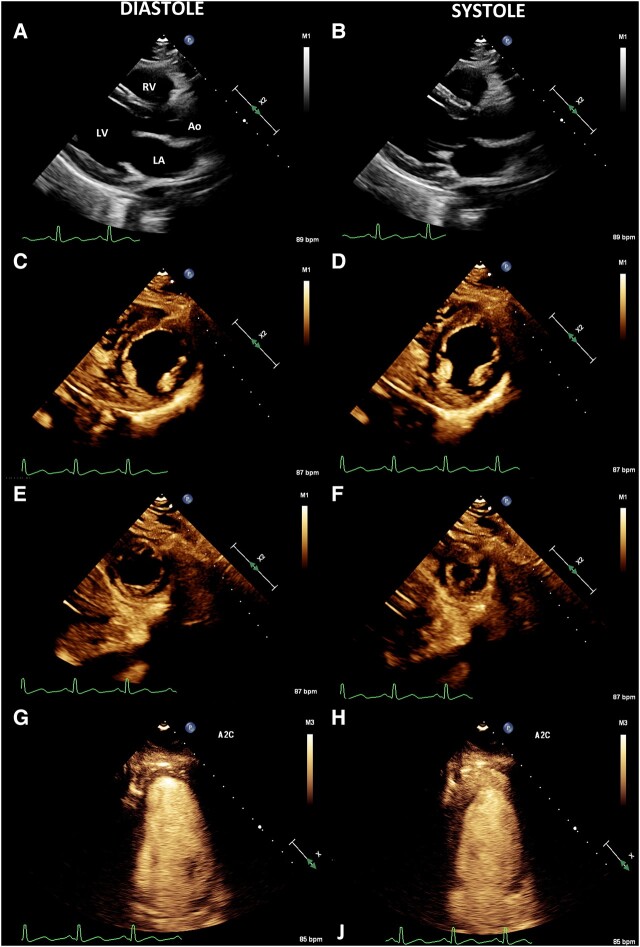
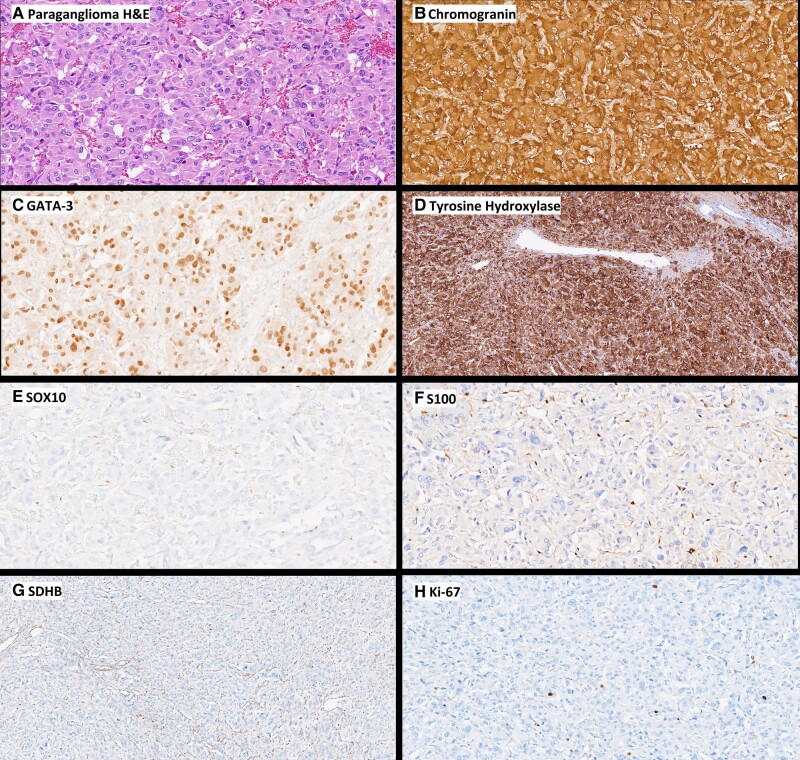
Background: Reverse takotsubo-like cardiomyopathy (rTCC) is a rare type of stress-induced cardiomyopathy associated with catecholamine surges. Reverse takotsubo-like cardiomyopathy is characterized by basal and mid-ventricular hypokinesis with apical sparing. Paragangliomas are catecholamine-secreting neuroendocrine tumours outside the adrenal gland that can cause palpitations, hypertension, and rarely cardiomyopathy. In cases of occult paraganglioma, catecholamine-induced rTCC can be rapidly reversed with adequate haemodynamic support.
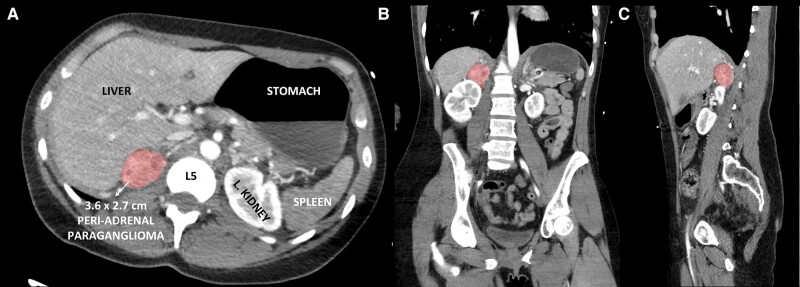
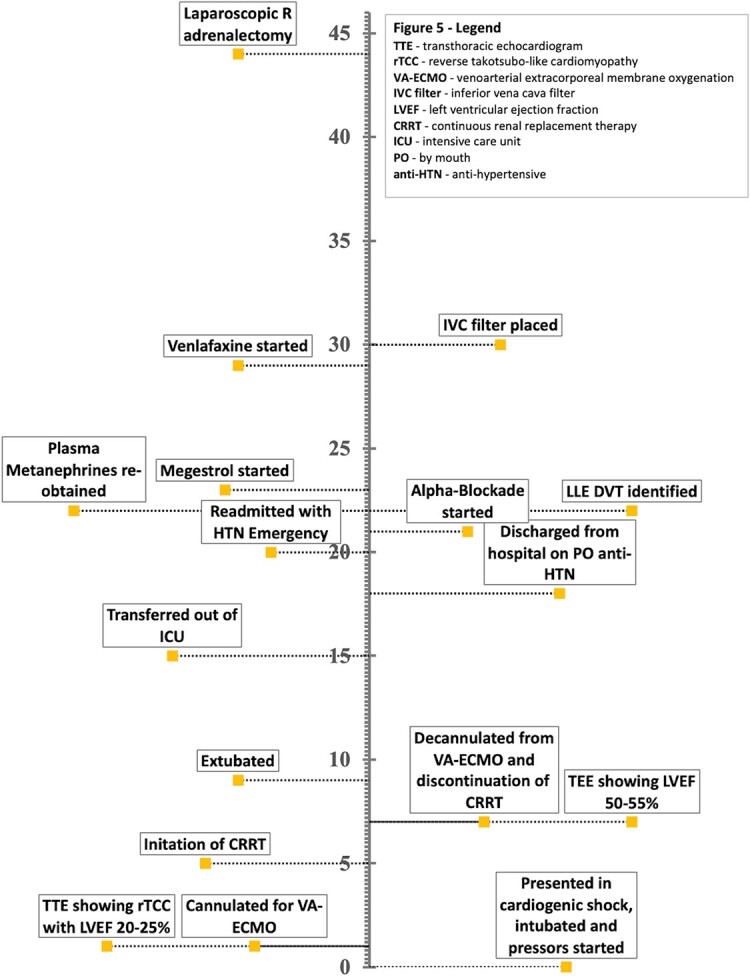
Case summary: A 28-year-old woman with a history of cervical cancer, ovarian insufficiency, and preeclampsia presented to the emergency department with nausea, vomiting, and chest pain. The patient was initially tachycardic, tachypnoeic, and hypotensive. On exam, she was in distress with diffuse rales and cool extremities. Electrocardiogram showed sinus tachycardia to 147 b.p.m. and lateral ST depression in V4 and V5. Troponin was elevated to 13 563 ng/L. An echocardiogram showed severely reduced left ventricular ejection fraction (LVEF) with hypokinesis of the basal segments and apical sparing, identified as rTCC. Computed tomography of the abdomen showed a 3.6 × 2.7 cm right adrenal mass. The patient rapidly developed respiratory failure and was subsequently intubated, sedated, and initiated on vasopressors. In the setting of cardiogenic shock refractory to vasopressor support, the decision was made to cannulate for venoarterial extracorporeal membrane oxygenation (VA-ECMO). Plasma and urine metanephrines were elevated. After 5 days, the patient's LVEF recovered to her baseline, and the rTCC had resolved. The patient's hypertension was managed with gradual alpha-blockade, and she subsequently underwent successful adrenalectomy on Day 44.
Discussion: An occult paraganglioma should be considered when rTCC pattern is identified. The pathophysiology of paraganglioma-mediated catecholamine surges predisposing to rTCC is unclear. Potential mechanisms for rTCC include oestrogen deficiency, catecholamine cardiotoxicity, and coronary artery spasm. The VA-ECMO is an increasingly used modality to provide haemodynamic support to patients with refractory cardiogenic shock.
Keywords: Cardiogenic shock; Case report; Extracorporeal membrane oxygenation; Paraganglioma; Reverse takotsubo cardiomyopathy; VA-ECMO.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures
References
-
- Khalid N, Ahmad SA, Shlofmitz E, Chhabra L. Pathophysiology of takotsubo syndrome [internet]. Statpearls. Treasure Island (FL): StatPearls Publishing; 2022. - PubMed
-
- Mete O, Asa SL, Gill AJ, Kimura N, de Krijger RR, Tischler A. Overview of the 2022 WHO classification of paragangliomas and pheochromocytomas. Endocr Pathol 2022;33:90–114. - PubMed
-
- Van Braeckel P, Carlier S, Steelant P-J, Weyne L, Vanfleteren L. Perioperative management of phaeochromocytoma. Acta Anaesthesiol Belg 2009;60:55–66. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous