

Comparison of Minimally Invasive Surgery with Open Surgery for Type II Endometrial Cancer: An Analysis of the National Cancer Database
- PMID: 38132012
- PMCID: PMC10743283
- DOI: 10.3390/healthcare11243122
Comparison of Minimally Invasive Surgery with Open Surgery for Type II Endometrial Cancer: An Analysis of the National Cancer Database
Abstract
Objective: Prior studies comparing minimally invasive surgery with open surgery among patients with endometrial cancer have reported similar survival outcomes and improved perioperative outcomes with minimally invasive surgery (MIS). However, patients with Type II endometrial cancer were underrepresented in these studies. We sought to compare the overall survival and surgical outcomes between open surgery and MIS in a large cohort of women with Type II endometrial cancer.
Methods: Using data from the National Cancer Database, we identified a cohort of women who underwent hysterectomy for type II endometrial cancer (serous, clear cell, and carcinosarcoma) between January 2010 and December 2014. The primary outcome was a comparison of the overall survival for MIS with that for the open approach. The secondary outcomes included a comparison of the length of hospital stay, readmission within 30 days of discharge, and 30- and 90-day mortality. Outcomes were compared between the cohorts using the Mann-Whitney U test, Pearson's chi-square test, or Fisher's exact test. Multivariable logistic regression with inverse propensity weighting was used to determine clinical characteristics that were statistically significant predictors of outcomes. p values < 0.05 were considered significant.
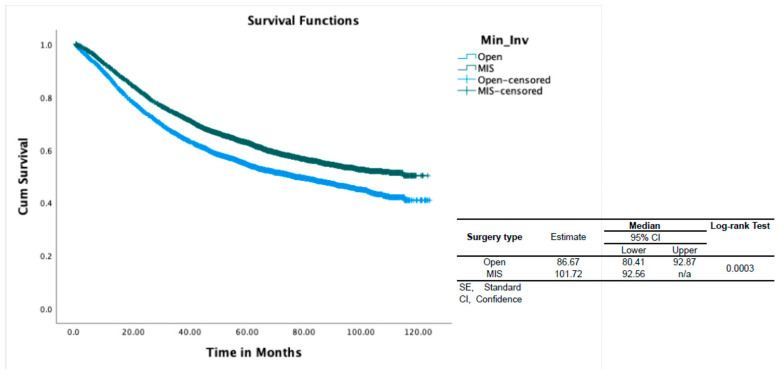
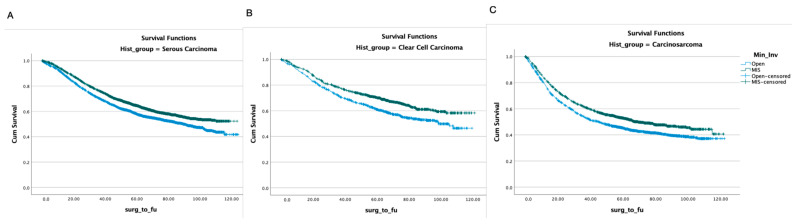
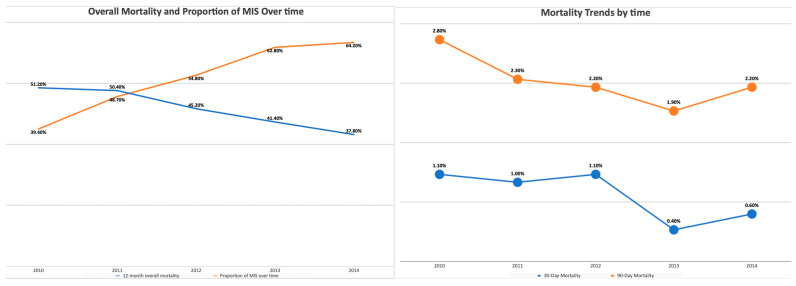
Results: We identified 12,905 patients with Type II, Stage I-III endometrial cancer that underwent a hysterectomy. In total, 7123 of these women (55.2%) underwent MIS. The rate of MIS increased from 39% to 64% over four years. Women who underwent MIS were more often White, privately insured, older, and had a higher income. The laparotomy group had a higher rate of carcinosarcoma histology (30.9% vs. 23.6%, p < 0.001), stage III disease (38.4% vs. 27.4%, p < 0.001), and larger primary tumors (59 vs. 45 mm, p < 0.001). Lymph node dissection was more commonly performed in the MIS group (89.6% vs. 85.4%, p < 0.001). With regard to adjuvant therapy, subjection to postoperative radiation was more common in the MIS group (37% vs. 40.1%, p < 0.001), while chemotherapy was more common in the laparotomy group (37.6% vs. 33.9%, p < 0.001). The time interval between surgery and the initiation of chemotherapy was shorter in the MIS group (39 vs. 42 days, p < 0.001). According to the results of propensity-score-weighted analysis, MIS was associated with superior overall survival (101.7 vs. 86.7 months, p = 0.0003 determined using the long-rank test), which corresponded to a 10% decreased risk of all-cause mortality (HR 0.9; CI 0.857-0.954, p = 0.0002). The survival benefit was uniform across all three histology types and stages. MIS was associated with superior perioperative outcomes, including shorter length of stay (1 vs. 4 days, p < 0.001), lower 30-day readmission rates (2.5% vs. 5%), and lower 30- and 90-day postoperative mortality (0.5% vs. 1.3% and 1.5% vs. 3.6%, respectively; p < 0.001 for both). The increased adoption of MIS from 2010 to 2014 corresponds to a decrease in 90-day postoperative mortality (2.8% to 2.2%, r = -0.89; p = 0.04) and overall mortality (51% to 38%, r = -0.95; p = 0.006).
Conclusions: In a large cohort of patients from the National Cancer Database, MIS was associated with improved overall survival and superior perioperative outcomes compared to open surgery among women with Type II endometrial cancer. A decrease in postoperative mortality and a shorter interval between surgery and the initiation of chemotherapy may contribute to the survival benefit of MIS. A racial and economic disparity in the surgical management of Type II endometrial cancer was identified, and further investigation is warranted to narrow this gap and improve patient outcomes.
Keywords: minimally invasive surgery; overall survival; type II endometrial cancer.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Impact of Robotic Assistance on Minimally Invasive Surgery for Type II Endometrial Cancer: A National Cancer Database Analysis.Cancers (Basel). 2024 Jul 19;16(14):2584. doi: 10.3390/cancers16142584. Cancers (Basel). 2024. PMID: 39061223 Free PMC article.
-
Conversion from Minimally Invasive Surgical Approaches to Open Surgery Among Patients with Endometrial Cancer in the SGO Clinical Outcomes Registry.Ann Surg Oncol. 2025 May;32(5):3458-3464. doi: 10.1245/s10434-025-16949-y. Epub 2025 Feb 21. Ann Surg Oncol. 2025. PMID: 39982547 Free PMC article.
-
Minimally invasive versus open surgery for women with stage 1A1 and stage 1A2 cervical cancer: A retrospective database cohort study.Ann Med Surg (Lond). 2022 Apr 7;77:103507. doi: 10.1016/j.amsu.2022.103507. eCollection 2022 May. Ann Med Surg (Lond). 2022. PMID: 35638032 Free PMC article.
-
Minimally invasive surgery versus open surgery in high-risk histologic endometrial cancer patients: A meta-analysis.Gynecol Oncol. 2022 Aug;166(2):236-244. doi: 10.1016/j.ygyno.2022.06.004. Epub 2022 Jun 17. Gynecol Oncol. 2022. PMID: 35725657
-
Surgical Treatment for Endometrial Cancer, Hysterectomy Performed via Minimally Invasive Routes Compared with Open Surgery: A Systematic Review and Network Meta-Analysis.Cancers (Basel). 2024 May 13;16(10):1860. doi: 10.3390/cancers16101860. Cancers (Basel). 2024. PMID: 38791939 Free PMC article. Review.
Cited by
-
Impact of Robotic Assistance on Minimally Invasive Surgery for Type II Endometrial Cancer: A National Cancer Database Analysis.Cancers (Basel). 2024 Jul 19;16(14):2584. doi: 10.3390/cancers16142584. Cancers (Basel). 2024. PMID: 39061223 Free PMC article.
References
-
- Walker J.L., Piedmonte M.R., Spirtos N.M., Eisenkop S.M., Schlaerth J.B., Mannel R.S., Spiegel G., Barakat R., Pearl M.L., Sharma S.K. Laparoscopy compared with laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group Study LAP2. J. Clin. Oncol. 2009;27:5331–5336. doi: 10.1200/JCO.2009.22.3248. - DOI - PMC - PubMed
-
- Janda M., Gebski V., Davies L.C., Forder P., Brand A., Hogg R., Jobling T.W., Land R., Manolitsas T., Nascimento M., et al. Effect of Total Laparoscopic Hysterectomy vs Total Abdominal Hysterectomy on Disease-Free Survival Among Women with Stage I Endometrial CancerA Randomized Clinical Trial. JAMA. 2017;317:1224–1233. doi: 10.1001/jama.2017.2068. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
