

The Role of Cone-Beam Computed Tomography CT Extremity Arthrography in the Preoperative Assessment of Osteoarthritis
- PMID: 38133071
- PMCID: PMC10747585
- DOI: 10.3390/tomography9060167
The Role of Cone-Beam Computed Tomography CT Extremity Arthrography in the Preoperative Assessment of Osteoarthritis
Abstract
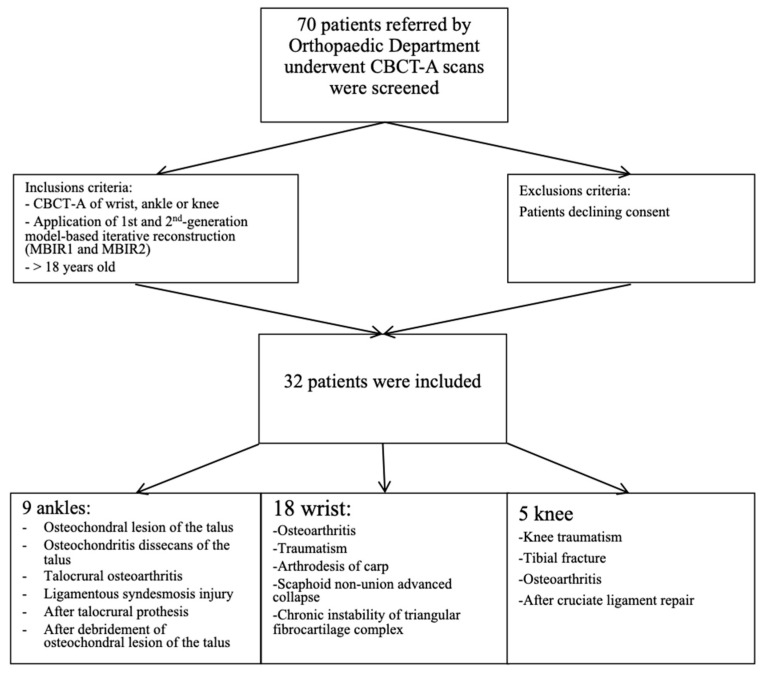
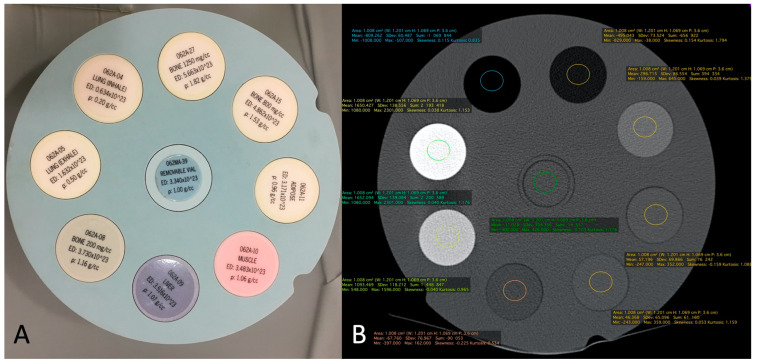
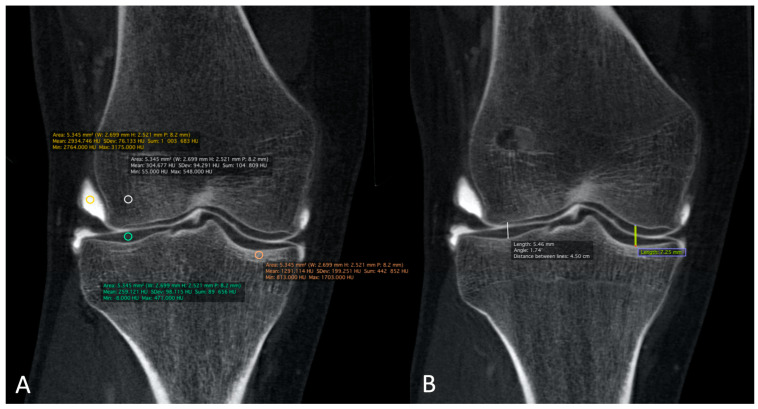
Osteoarthritis (OA) is a prevalent disease and the leading cause of pain, disability, and quality of life deterioration. Our study sought to evaluate the image quality and dose of cone-beam computed tomography arthrography (CBCT-A) and compare them to digital radiography (DR) for OA diagnoses. Overall, 32 cases of CBCT-A and DR with OA met the inclusion criteria and were prospectively analyzed. The Kellgren and Lawrence classification (KLC) stage, sclerosis, osteophytes, erosions, and mean joint width (MJW) were compared between CBCT-A and DR. Image quality was excellent in all CBCT-A cases, with excellent inter-observer agreement. OA under-classification was noticed with DR for MJW (p = 0.02), osteophyte detection (<0.0001), and KLC (p < 0.0001). The Hounsfield Unit (HU) values obtained for the cone-beam computed tomography CBCT did not correspond to the values for multi-detector computed tomography (MDCT), with a greater mean deviation obtained with the MDCT HU for Modeled Based Iterative Reconstruction 1st (MBIR1) than for the 2nd generation (MBIR2). CBCT-A has been found to be more reliable for OA diagnosis than DR as revealed by our results using a three-point rating scale for the qualitative image analysis, with higher quality and an acceptable dose. Moreover, the use of this imaging technique permits the preoperative assessment of extremities in an OA diagnosis, with the upright position and bone microarchitecture analysis being two other advantages of CBCT-A.
Keywords: Kellgren and Lawrence classification; X-ray; cone-beam computed tomography arthrography; density; osteoarthritis; radiation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Experiences with image quality and radiation dose of cone beam computed tomography (CBCT) and multidetector computed tomography (MDCT) in pediatric extremity trauma.Skeletal Radiol. 2020 Dec;49(12):1939-1949. doi: 10.1007/s00256-020-03506-9. Epub 2020 Jun 14. Skeletal Radiol. 2020. PMID: 32535775 Free PMC article.
-
Performance of cone-beam computed tomography and multidetector computed tomography in diagnostic imaging of the midface: A comparative study on Phantom and cadaver head scans.Eur Radiol. 2017 Feb;27(2):790-800. doi: 10.1007/s00330-016-4387-2. Epub 2016 May 11. Eur Radiol. 2017. PMID: 27169574
-
Using cone-beam CT as a low-dose 3D imaging technique for the extremities: initial experience in 50 subjects.Skeletal Radiol. 2015 Jun;44(6):797-809. doi: 10.1007/s00256-015-2105-9. Epub 2015 Feb 5. Skeletal Radiol. 2015. PMID: 25652734
-
Using Cone Beam Computed Tomography for Radiological Assessment Beyond Dento-maxillofacial Imaging: A Review of the Clinical Applications in other Anatomical Districts.Curr Med Imaging. 2023;19(9):977-994. doi: 10.2174/1573405619666230202122947. Curr Med Imaging. 2023. PMID: 36733238 Review.
-
Are multi-detector computed tomography and cone-beam computed tomography exams and software accurate to measure the upper airway? A systematic review.Eur J Orthod. 2023 Nov 30;45(6):818-831. doi: 10.1093/ejo/cjad060. Eur J Orthod. 2023. PMID: 37797294
Cited by
-
Cone beam CT in the imaging of musculoskeletal trauma: a scoping review.Skeletal Radiol. 2025 Oct;54(10):1997-2005. doi: 10.1007/s00256-025-04947-w. Epub 2025 May 14. Skeletal Radiol. 2025. PMID: 40369229 Free PMC article. Review.
References
-
- Hayashi D., Guermazi A., Crema M.D., Roemer F.W. Imaging in osteoarthritis: What have we learned and where are we going? Minerva Med. 2011;102:15–32. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
