

Surgical Management of Traumatic Meniscus Injuries
- PMID: 38133145
- PMCID: PMC10747583
- DOI: 10.3390/pathophysiology30040044
Surgical Management of Traumatic Meniscus Injuries
Abstract
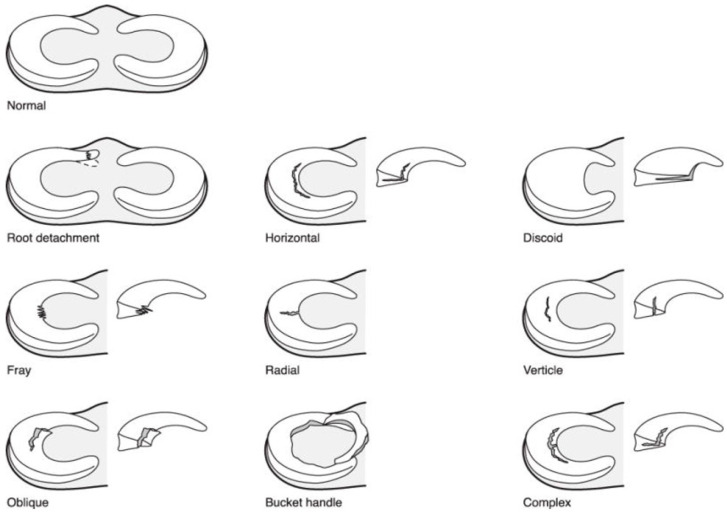
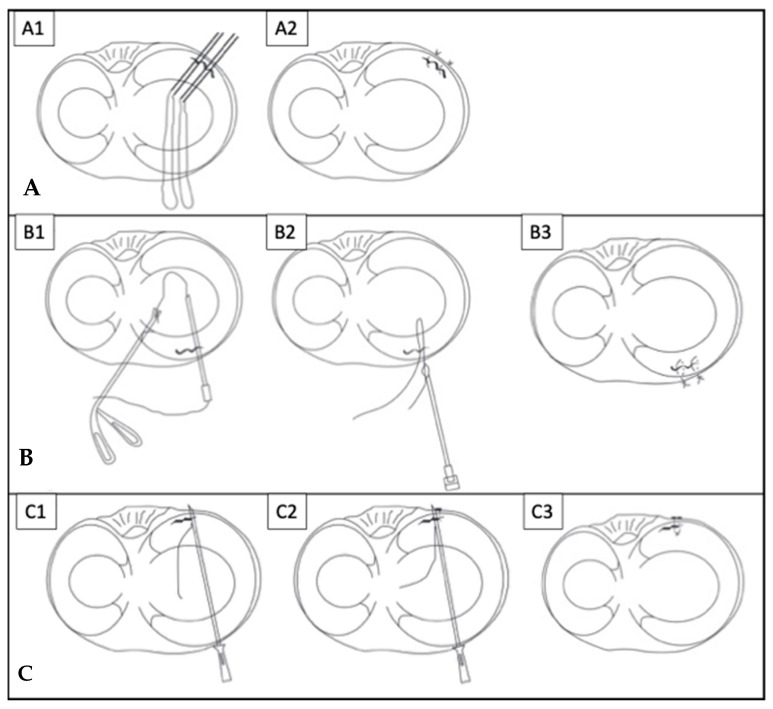
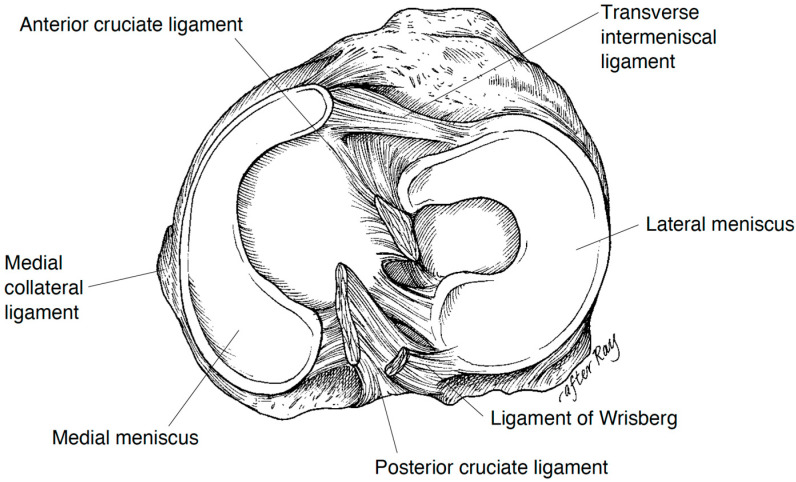
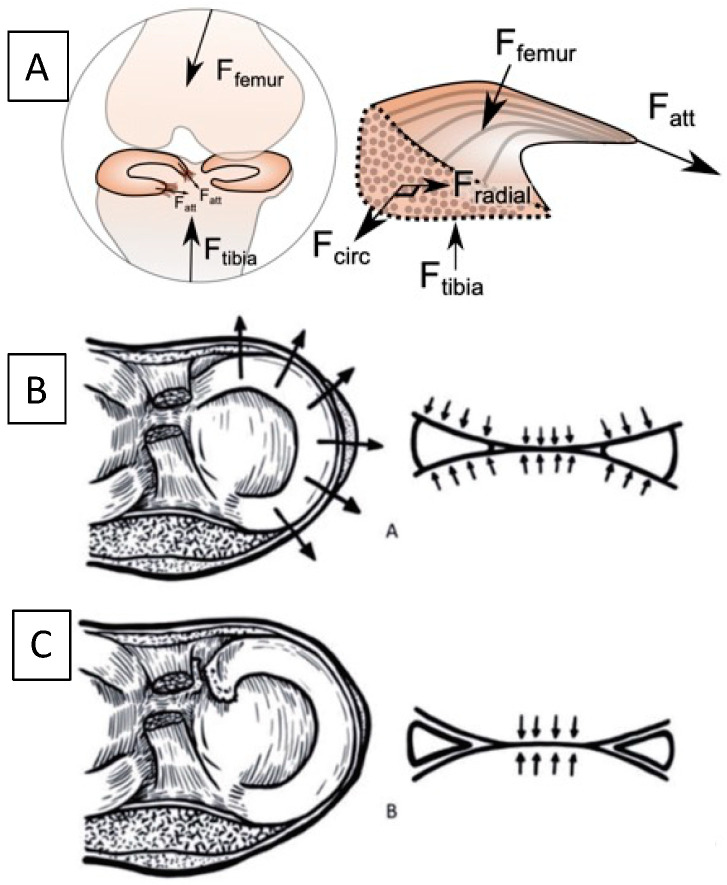
The menisci increase the contact area of load bearing in the knee and thus disperse the mechanical stress via their circumferential tensile fibers. Traumatic meniscus injuries cause mechanical symptoms in the knee, and are more prevalent amongst younger, more active patients, compared to degenerative tears amongst the elderly population. Traumatic meniscus tears typically result from the load-and-shear mechanism in the knee joint. The treatment depends on the size, location, and pattern of the tear. For non-repairable tears, partial or total meniscal resection decreases its tensile stress and increases joint contact stress, thus potentiating the risk of arthritis. A longitudinal vertical tear pattern at the peripheral third red-red zone leads to higher healing potential after repair. The postoperative rehabilitation protocols after repair range from immediate weight-bearing with no range of motion restrictions to non-weight bearing and delayed mobilization for weeks. Pediatric and adolescent patients may require special considerations due to their activity levels, or distinct pathologies such as a discoid meniscus. Further biomechanical and biologic evidence is needed to guide surgical management, postoperative rehabilitation protocols, and future technology applications for traumatic meniscus injuries.
Keywords: knee biomechanics; knee rehabilitation; meniscus repair; meniscus tear; orthopaedics; sports medicine.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources