

Association between carotenoid intake and metabolic dysfunction-associated fatty liver disease among US adults: A cross-sectional study
- PMID: 38134087
- PMCID: PMC10735096
- DOI: 10.1097/MD.0000000000036658
Association between carotenoid intake and metabolic dysfunction-associated fatty liver disease among US adults: A cross-sectional study
Abstract
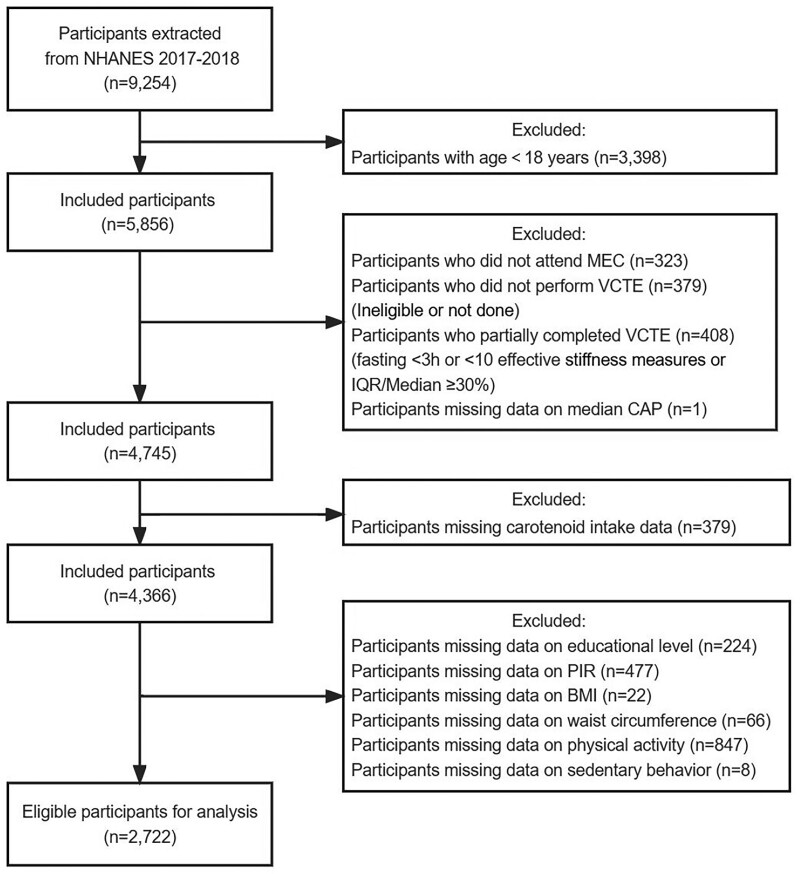
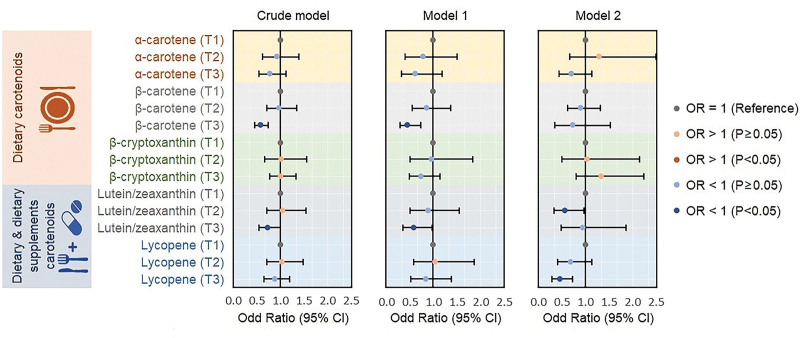
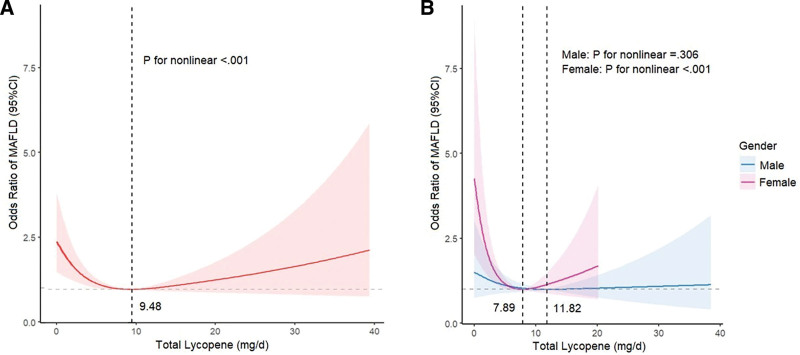
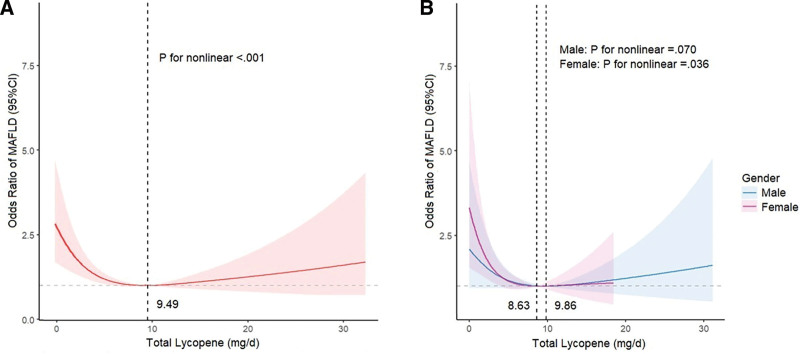
Carotenoids have been recognized for their potential health benefits due to their antioxidant properties. There is limited research on the association between metabolic dysfunction-associated fatty liver disease (MAFLD) and carotenoids. This study aimed to investigate the effect of carotenoid intake on the risk of MAFLD. We retrospectively analyzed 2722 adults aged ≥ 18 from the National Health and Nutrition Examination Survey 2017-2018. Hepatic steatosis was identified by elastography, and carotenoid consumption was evaluated through two 24-hour dietary recall interviews. Weighted logistic regression models, subgroup analyses, and restricted cubic splines were used for analyses. The weighted prevalence of MAFLD was 51.90%. Weighted logistic regression analysis demonstrated that intake of β-carotene, lutein/zeaxanthin, and lycopene was associated with a lower risk of MAFLD after adjusting for various covariates. Compared to the lowest tertile, a significant inverse correlation was observed between the highest total lycopene intake and MAFLD among females in the gender subgroup analysis. Restricted cubic spline regression analysis revealed a U-shaped association between lycopene consumption and MAFLD risk (P < .001), with an inflection point of approximately 9.48 mg/day. Moreover, the nonlinear relationship was particularly significant in females and absent in males. In summary, increased β-carotene, lutein/zeaxanthin, and lycopene consumption was associated with a decreased risk of MAFLD. The relationship between total lycopene intake and MAFLD was nonlinear, primarily in females. These findings have significant implications for the potential prevention and management of MAFLD.
Copyright © 2023 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
Similar articles
-
Association between dietary intake of carotenoids and metabolic dysfunction-associated fatty liver disease in US adults: National Health and Nutrition Examination Survey 2017-March 2020.Public Health Nutr. 2024 Sep 24;27(1):e168. doi: 10.1017/S1368980024001502. Public Health Nutr. 2024. PMID: 39313756 Free PMC article.
-
Associations of serum carotenoids with all-cause and cardiovascular mortality in adults with MAFLD.Nutr Metab Cardiovasc Dis. 2024 Oct;34(10):2315-2324. doi: 10.1016/j.numecd.2024.06.001. Epub 2024 Jun 6. Nutr Metab Cardiovasc Dis. 2024. PMID: 39003130
-
Serum carotenoid levels inversely correlate with depressive symptoms among adults: Insights from NHANES data.J Affect Disord. 2024 Oct 1;362:869-876. doi: 10.1016/j.jad.2024.07.021. Epub 2024 Jul 24. J Affect Disord. 2024. PMID: 39025444
-
Carotenoid Intake and Circulating Carotenoids Are Inversely Associated with the Risk of Bladder Cancer: A Dose-Response Meta-analysis.Adv Nutr. 2020 May 1;11(3):630-643. doi: 10.1093/advances/nmz120. Adv Nutr. 2020. PMID: 31800007 Free PMC article.
-
Systematic review of carotenoid concentrations in human milk and infant blood.Nutr Rev. 2022 Aug 8;80(9):2029-2050. doi: 10.1093/nutrit/nuac018. Nutr Rev. 2022. PMID: 35389473
Cited by
-
Association Between Lycopene and Metabolic Disease Risk and Mortality: Systematic Review and Meta-Analysis.Life (Basel). 2025 Jun 12;15(6):944. doi: 10.3390/life15060944. Life (Basel). 2025. PMID: 40566597 Free PMC article. Review.
-
Lutein Production and Extraction from Microalgae: Recent Insights and Bioactive Potential.Int J Mol Sci. 2024 Mar 1;25(5):2892. doi: 10.3390/ijms25052892. Int J Mol Sci. 2024. PMID: 38474137 Free PMC article. Review.
References
-
- Eslam M, Newsome PN, Sarin SK, et al. . A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73:202–9. - PubMed
-
- Lim GEH, Tang A, Ng CH, et al. . An observational data meta-analysis on the differences in prevalence and risk factors between MAFLD vs NAFLD. Clin Gastroenterol Hepatol. 2023;21:619–629.e7. - PubMed
-
- Ciardullo S, Perseghin G. Prevalence of NAFLD, MAFLD and associated advanced fibrosis in the contemporary United States population. Liver Int. 2021;41:1290–3. - PubMed
-
- Kim D, Konyn P, Sandhu KK, et al. . Metabolic dysfunction-associated fatty liver disease is associated with increased all-cause mortality in the United States. J Hepatol. 2021;75:1284–91. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
