Trial Readiness of Cavernous Malformations With Symptomatic Hemorrhage, Part II: Biomarkers and Trial Modeling
- PMID: 38134265
- PMCID: PMC10752356
- DOI: 10.1161/STROKEAHA.123.044083
Trial Readiness of Cavernous Malformations With Symptomatic Hemorrhage, Part II: Biomarkers and Trial Modeling
Abstract
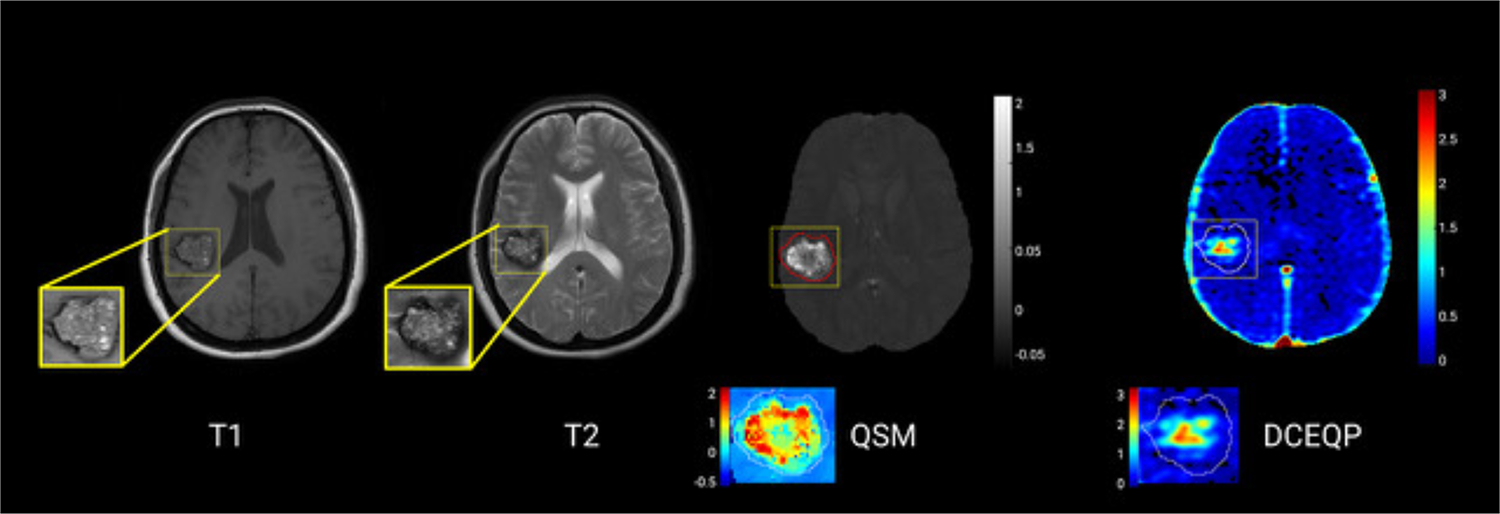
Background: Quantitative susceptibility mapping (QSM) and dynamic contrast-enhanced quantitative perfusion (DCEQP) magnetic resonance imaging sequences assessing iron deposition and vascular permeability were previously correlated with new hemorrhage in cerebral cavernous malformations. We assessed their prospective changes in a multisite trial-readiness project.
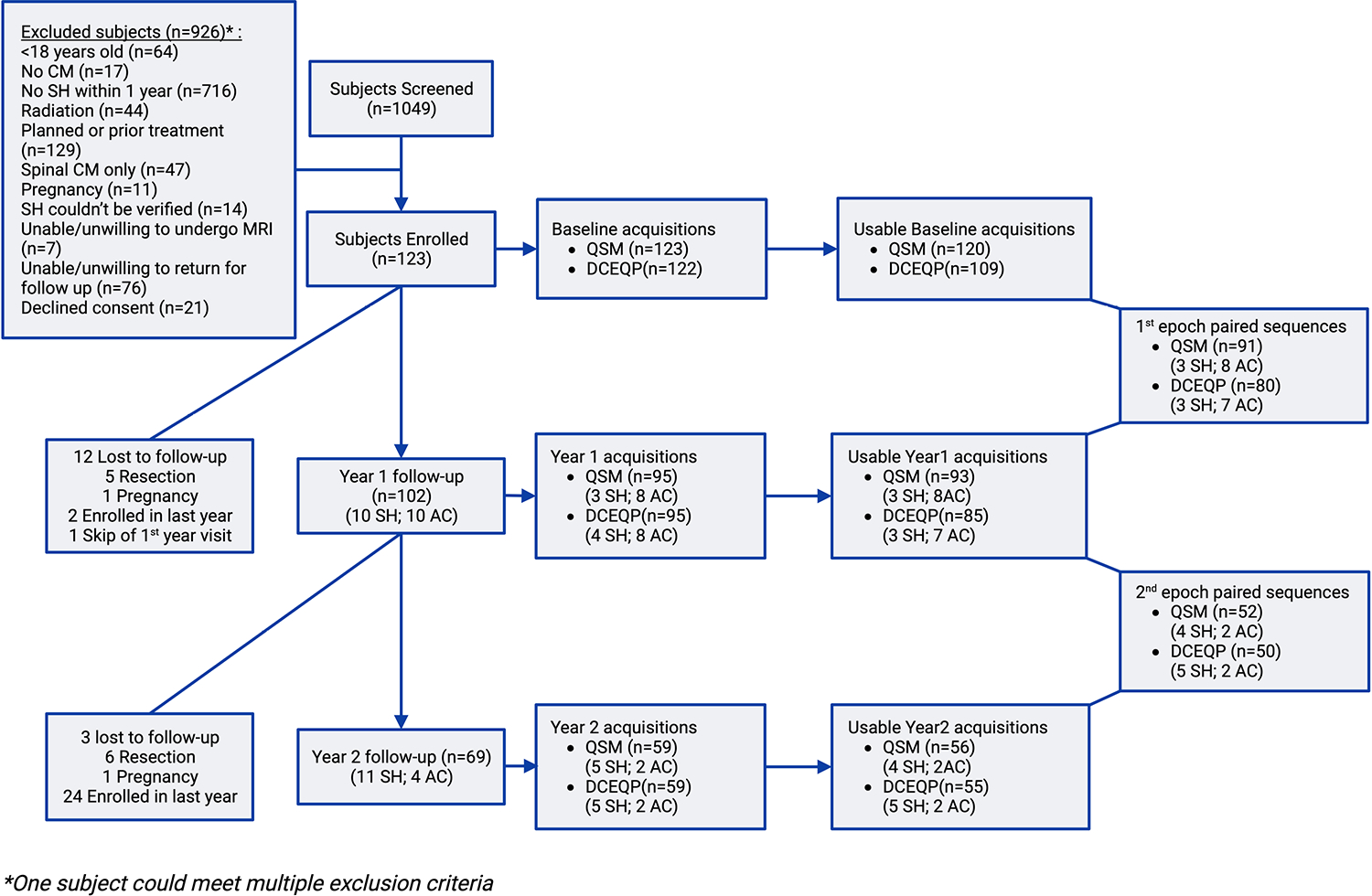
Methods: Patients with cavernous malformation and symptomatic hemorrhage (SH) in the prior year, without prior or planned lesion resection or irradiation were enrolled. Mean QSM and DCEQP of the SH lesion were acquired at baseline and at 1- and 2-year follow-ups. Sensitivity and specificity of biomarker changes were analyzed in relation to predefined criteria for recurrent SH or asymptomatic change. Sample size calculations for hypothesized therapeutic effects were conducted.
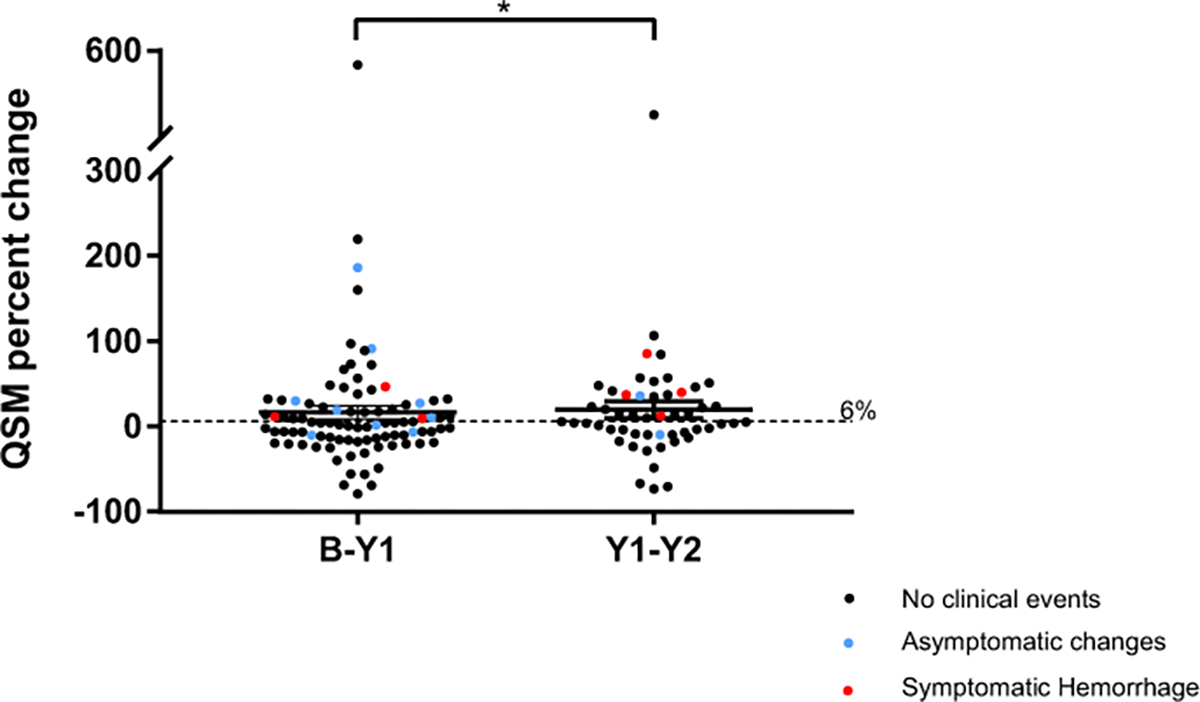
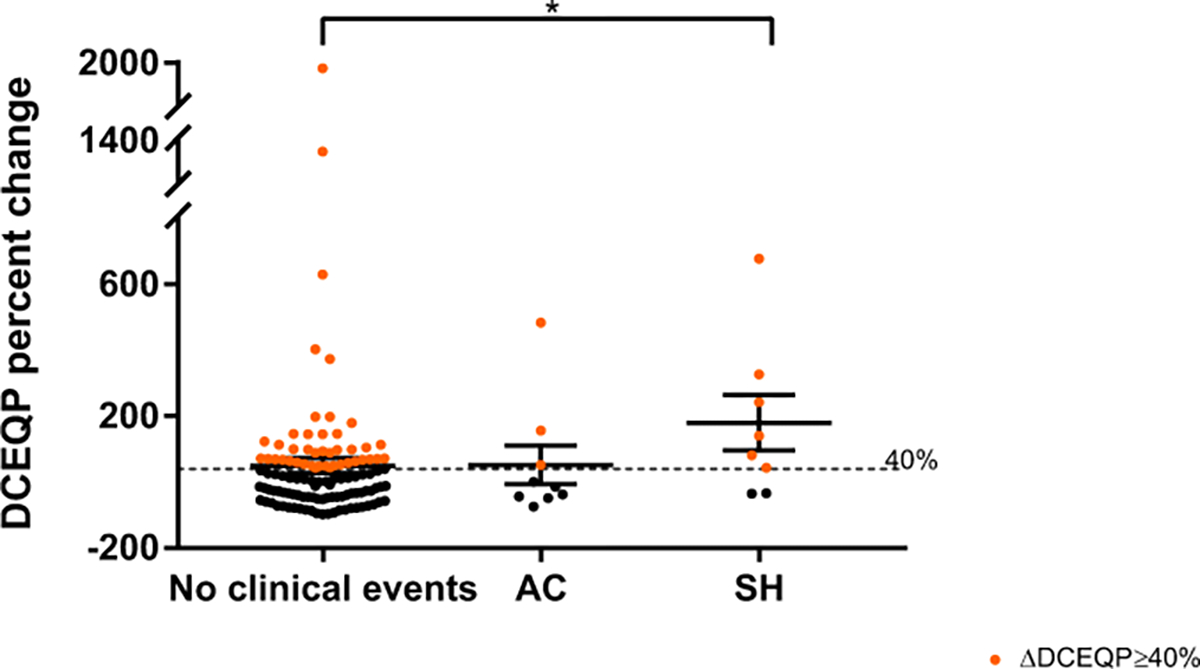
Results: We logged 143 QSM and 130 DCEQP paired annual assessments. Annual QSM change was greater in cases with SH than in cases without SH (P=0.019). Annual QSM increase by ≥6% occurred in 7 of 7 cases (100%) with recurrent SH and in 7 of 10 cases (70%) with asymptomatic change during the same epoch and 3.82× more frequently than clinical events. DCEQP change had lower sensitivity for SH and asymptomatic change than QSM change and greater variance. A trial with the smallest sample size would detect a 30% difference in QSM annual change during 2 years of follow-up in 34 or 42 subjects (1 and 2 tailed, respectively); power, 0.8, α=0.05.
Conclusions: Assessment of QSM change is feasible and sensitive to recurrent bleeding in cavernous malformations. Evaluation of an intervention on QSM percent change may be used as a time-averaged difference between 2 arms using a repeated measures analysis. DCEQP change is associated with lesser sensitivity and higher variability than QSM. These results are the basis of an application for certification by the US Food and Drug Administration of QSM as a biomarker of drug effect on bleeding in cavernous malformations.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT03652181.
Keywords: biomarkers; hemorrhage; iron; perfusion; permeability.
Conflict of interest statement
Figures