

Concomitant Administration of Ad26.RSV.preF/RSV preF Protein Vaccine and High-Dose Influenza Vaccine in Adults 65 Years and Older: A Noninferiority Trial
- PMID: 38134393
- PMCID: PMC11326816
- DOI: 10.1093/infdis/jiad594
Concomitant Administration of Ad26.RSV.preF/RSV preF Protein Vaccine and High-Dose Influenza Vaccine in Adults 65 Years and Older: A Noninferiority Trial
Abstract
Background: Since influenza and respiratory syncytial virus (RSV) carry significant burden in older adults with overlapping seasonality, vaccines for both pathogens would ideally be coadministered in this population. Here we evaluate the immunogenicity and safety of concomitant administration of Ad26.RSV.preF/RSV preF protein and high-dose seasonal influenza vaccine (Fluzone-HD) in adults ≥65 years old.
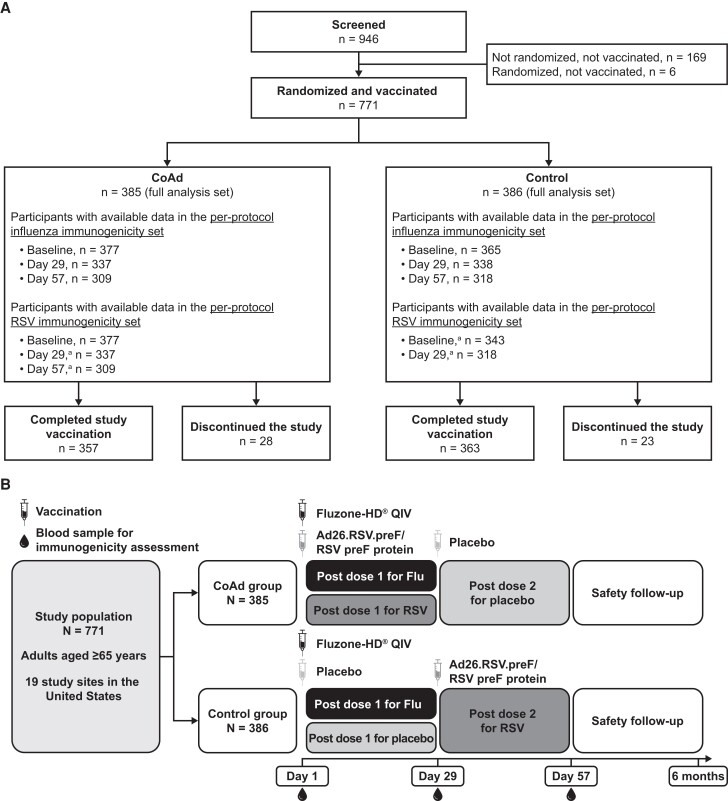
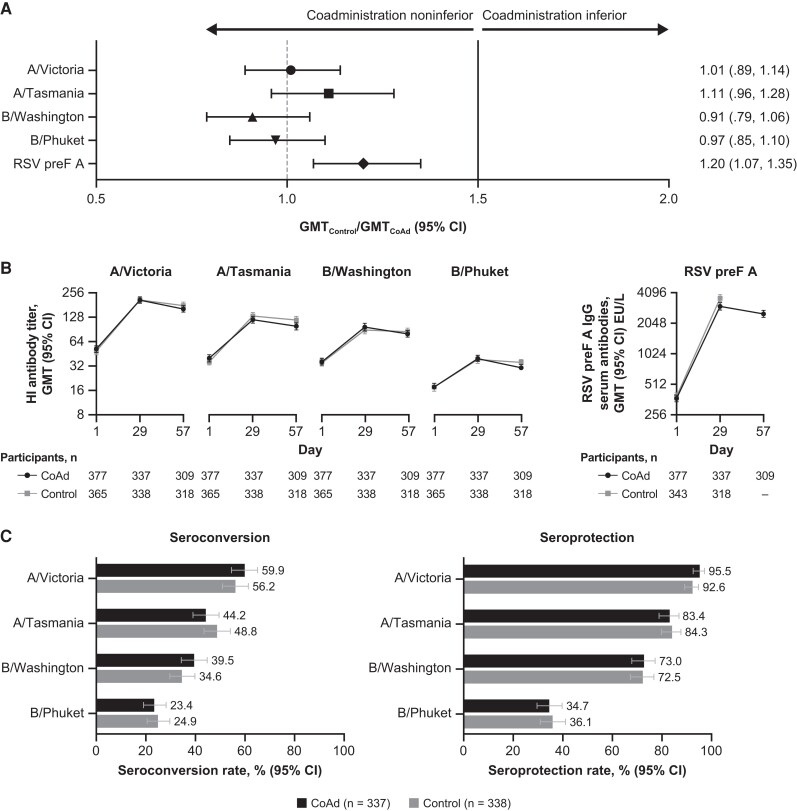
Methods: Participants were randomized 1:1 to the Coadministration or Control group. The Coadministration group received concomitant Ad26.RSV.preF/RSV preF protein and Fluzone-HD on day 1 and placebo on day 29, while the Control group received Fluzone-HD and placebo on day 1 and Ad26.RSV.preF/RSV preF protein on day 29. Influenza hemagglutination-inhibiting and RSV preF-binding antibody titers were measured postvaccination and tested for noninferiority between both groups. Safety data were collected throughout the study and analyzed descriptively.
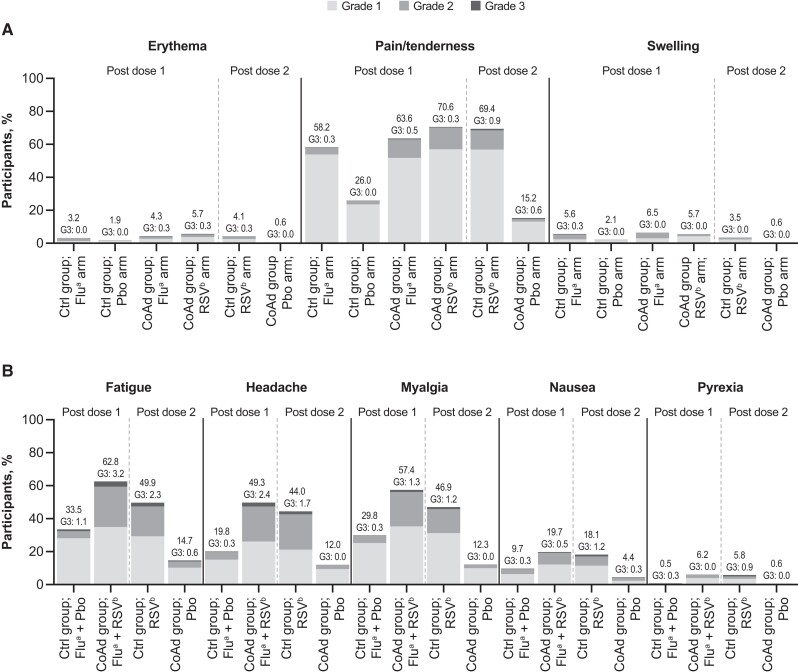
Results: Coadministered Ad26.RSV.preF/RSV preF protein and Fluzone-HD vaccines induced noninferior immune responses compared to each vaccine administered alone. Seroconversion and seroprotection rates against influenza were similar between groups. Both vaccines remained well tolerated upon concomitant administration.
Conclusions: Coadministration of Ad26.RSV.preF/RSV preF protein and Fluzone-HD showed an acceptable safety profile and did not hamper the immunogenicity of either vaccine, thus supporting that both vaccines can be concomitantly administered in adults ≥65 years old.
Keywords: Ad26.RSV.preF/RSV preF protein; Fluzone-HD; influenza; noninferiority; respiratory syncytial virus.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. W. W., C. A. C., and E. H. are former employees of Janssen Vaccines and Prevention B.V.; A. R. B., N. L., and B. C. are employees of Janssen Vaccines and Prevention B.V.; A. M. J. and I. S. are employees of Janssen Research and Development; E. D. P. is a former employee of Janssen Infectious Diseases. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Shi T, Denouel A, Tietjen AK, et al. . Global disease burden estimates of respiratory syncytial virus–associated acute respiratory infection in older adults in 2015: a systematic review and meta-analysis. J Infect Dis 2020; 222:S577–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
