

Microbiome preterm birth DREAM challenge: Crowdsourcing machine learning approaches to advance preterm birth research
- PMID: 38134931
- PMCID: PMC10829755
- DOI: 10.1016/j.xcrm.2023.101350
Microbiome preterm birth DREAM challenge: Crowdsourcing machine learning approaches to advance preterm birth research
Abstract
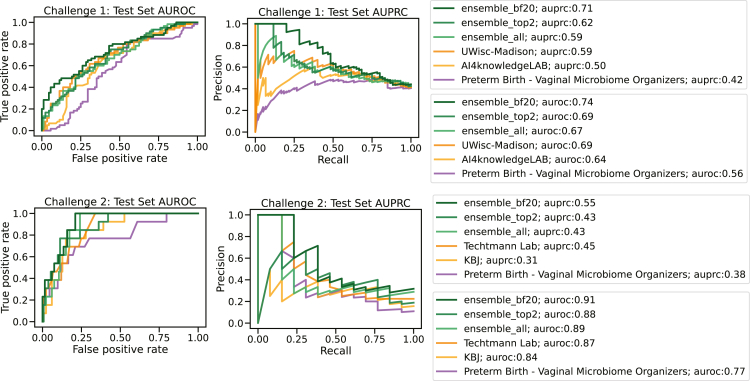
Every year, 11% of infants are born preterm with significant health consequences, with the vaginal microbiome a risk factor for preterm birth. We crowdsource models to predict (1) preterm birth (PTB; <37 weeks) or (2) early preterm birth (ePTB; <32 weeks) from 9 vaginal microbiome studies representing 3,578 samples from 1,268 pregnant individuals, aggregated from public raw data via phylogenetic harmonization. The predictive models are validated on two independent unpublished datasets representing 331 samples from 148 pregnant individuals. The top-performing models (among 148 and 121 submissions from 318 teams) achieve area under the receiver operator characteristic (AUROC) curve scores of 0.69 and 0.87 predicting PTB and ePTB, respectively. Alpha diversity, VALENCIA community state types, and composition are important features in the top-performing models, most of which are tree-based methods. This work is a model for translation of microbiome data into clinically relevant predictive models and to better understand preterm birth.
Keywords: 16S harmonization; DREAM challenge; crowdsourced; machine learning; microbiome; predictive modeling; preterm birth; vaginal microbiome.
Copyright © 2023 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests S.V.L. is a board member at, holds stock in, and consults for Siolta Therapeutics. She also consults for the Atria Academy of Science and Medicine and for Sanofi. J.C.C. is co-founder of PrecisionProfile and OncoRx Insights. N.Aghaeepour. is a member of the scientific advisory boards of January AI, Parallel Bio, Celine Therapeutics, and WellSim Biomedical Technologies and is a paid consultant for Mara BioSystems. J.G. and M.S. have filed a patent related to the phylotype generation process.
Figures





Update of
-
Microbiome Preterm Birth DREAM Challenge: Crowdsourcing Machine Learning Approaches to Advance Preterm Birth Research.medRxiv [Preprint]. 2023 Apr 11:2023.03.07.23286920. doi: 10.1101/2023.03.07.23286920. medRxiv. 2023. Update in: Cell Rep Med. 2024 Jan 16;5(1):101350. doi: 10.1016/j.xcrm.2023.101350. PMID: 36945505 Free PMC article. Updated. Preprint.
References
-
- Blencowe H., Cousens S., Oestergaard M.Z., Chou D., Moller A.-B., Narwal R., Adler A., Vera Garcia C., Rohde S., Say L., Lawn J.E. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379:2162–2172. - PubMed
-
- Liu L., Johnson H.L., Cousens S., Perin J., Scott S., Lawn J.E., Rudan I., Campbell H., Cibulskis R., Li M., et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151–2161. - PubMed
-
- Lynch A.M., Hart J.E., Agwu O.C., Fisher B.M., West N.A., Gibbs R.S. Association of extremes of prepregnancy BMI with the clinical presentations of preterm birth. Am. J. Obstet. Gynecol. 2014;210:428.e1–428.e9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
