

The burden of bacterial antimicrobial resistance in the WHO African region in 2019: a cross-country systematic analysis
- PMID: 38134946
- PMCID: PMC10805005
- DOI: 10.1016/S2214-109X(23)00539-9
The burden of bacterial antimicrobial resistance in the WHO African region in 2019: a cross-country systematic analysis
Abstract
Background: A critical and persistent challenge to global health and modern health care is the threat of antimicrobial resistance (AMR). Previous studies have reported a disproportionate burden of AMR in low-income and middle-income countries, but there remains an urgent need for more in-depth analyses across Africa. This study presents one of the most comprehensive sets of regional and country-level estimates of bacterial AMR burden in the WHO African region to date.
Methods: We estimated deaths and disability-adjusted life-years (DALYs) attributable to and associated with AMR for 23 bacterial pathogens and 88 pathogen-drug combinations for countries in the WHO African region in 2019. Our methodological approach consisted of five broad components: the number of deaths in which infection had a role, the proportion of infectious deaths attributable to a given infectious syndrome, the proportion of infectious syndrome deaths attributable to a given pathogen, the percentage of a given pathogen resistant to an antimicrobial drug of interest, and the excess risk of mortality (or duration of an infection) associated with this resistance. These components were then used to estimate the disease burden by using two counterfactual scenarios: deaths attributable to AMR (considering an alternative scenario where infections with resistant pathogens are replaced with susceptible ones) and deaths associated with AMR (considering an alternative scenario where drug-resistant infections would not occur at all). We obtained data from research hospitals, surveillance networks, and infection databases maintained by private laboratories and medical technology companies. We generated 95% uncertainty intervals (UIs) for final estimates as the 25th and 975th ordered values across 1000 posterior draws, and models were cross-validated for out-of-sample predictive validity.
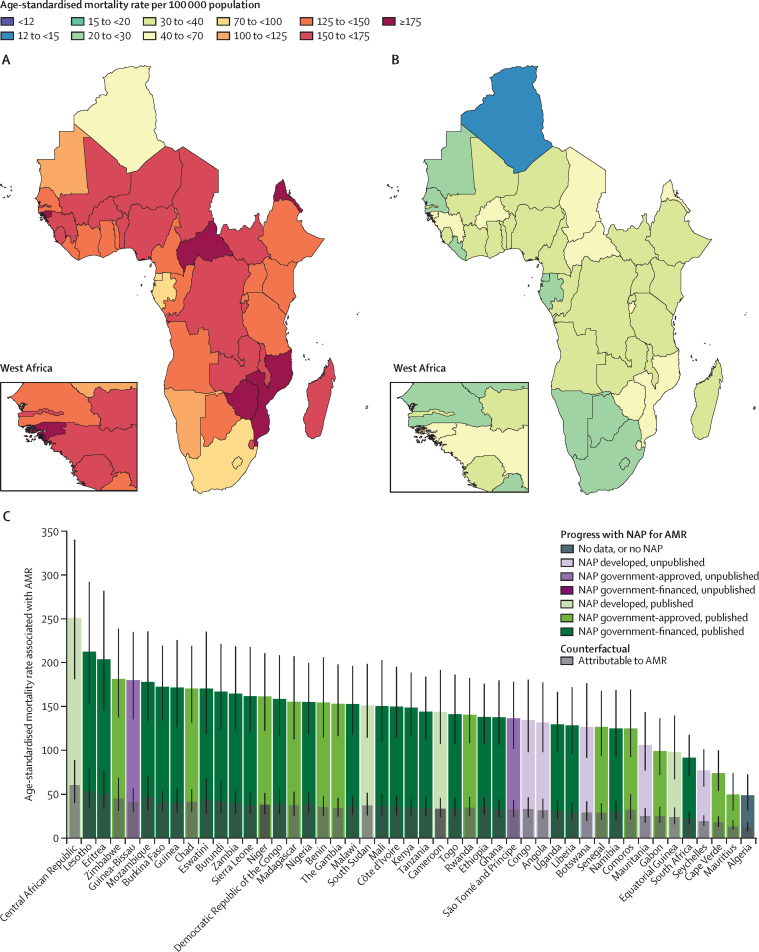
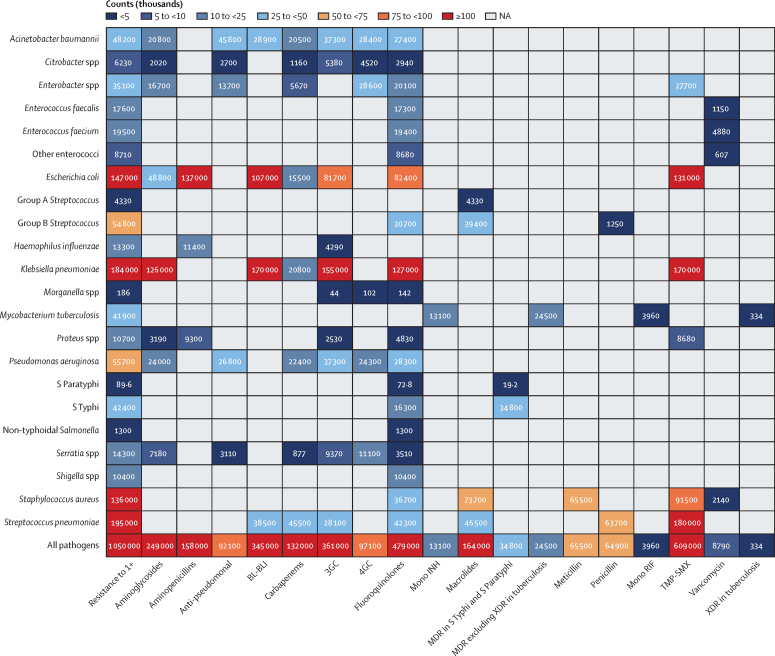
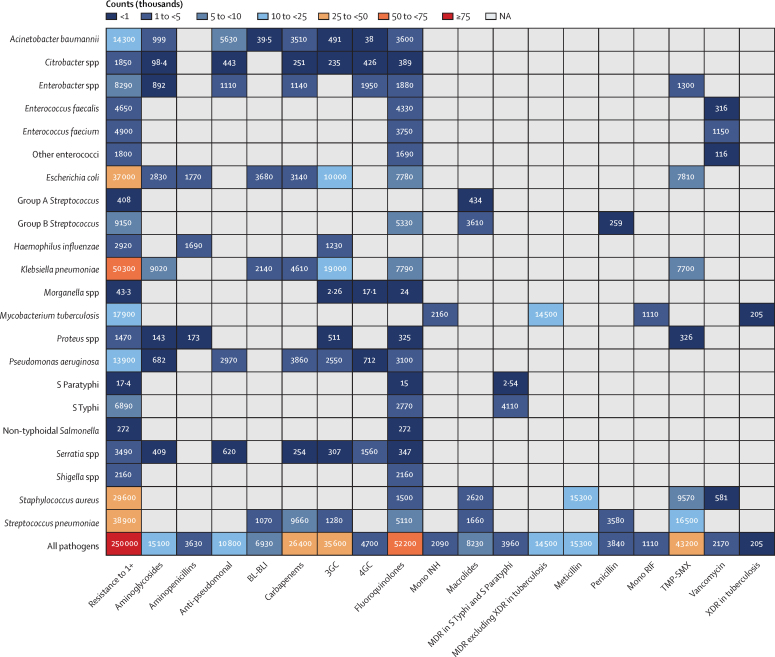
Findings: In the WHO African region in 2019, there were an estimated 1·05 million deaths (95% UI 829 000-1 316 000) associated with bacterial AMR and 250 000 deaths (192 000-325 000) attributable to bacterial AMR. The largest fatal AMR burden was attributed to lower respiratory and thorax infections (119 000 deaths [92 000-151 000], or 48% of all estimated bacterial pathogen AMR deaths), bloodstream infections (56 000 deaths [37 000-82 000], or 22%), intra-abdominal infections (26 000 deaths [17 000-39 000], or 10%), and tuberculosis (18 000 deaths [3850-39 000], or 7%). Seven leading pathogens were collectively responsible for 821 000 deaths (636 000-1 051 000) associated with resistance in this region, with four pathogens exceeding 100 000 deaths each: Streptococcus pneumoniae, Klebsiella pneumoniae, Escherichia coli, and Staphylococcus aureus. Third-generation cephalosporin-resistant K pneumoniae and meticillin-resistant S aureus were shown to be the leading pathogen-drug combinations in 25 and 16 countries, respectively (53% and 34% of the whole region, comprising 47 countries) for deaths attributable to AMR.
Interpretation: This study reveals a high level of AMR burden for several bacterial pathogens and pathogen-drug combinations in the WHO African region. The high mortality rates associated with these pathogens demonstrate an urgent need to address the burden of AMR in Africa. These estimates also show that quality and access to health care and safe water and sanitation are correlated with AMR mortality, with a higher fatal burden found in lower resource settings. Our cross-country analyses within this region can help local governments to leverage domestic and global funding to create stewardship policies that target the leading pathogen-drug combinations.
Funding: Bill & Melinda Gates Foundation, Wellcome Trust, and Department of Health and Social Care using UK aid funding managed by the Fleming Fund.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests E Chung reports support for the present manuscript from the National Institutes of Health, training grant NICHD T32HD007233. S J Dunachie reports support for the present manuscript from the UK Fleming Fund at the Department of Health and Social Care, the Bill & Melinda Gates Foundation, and the Wellcome Trust; grants or contracts from the UK National Institute for Health and Care Research (NIHR); participation on a Data Safety Monitoring Committee for the UK STABILISE study of BCG vaccine in COPD as a committee member; and leadership or fiduciary roles in board, society, committee or advocacy groups, as a paid member of the Wellcome Trust Vaccines Advisory Selection Panel for “Vaccines and AMR” (November, 2019), a paid member of the Interview Committee of the Wellcome Early Career Awards (2022–25), an unpaid expert advisor to WHO's Global Antimicrobial Resistance Surveillance System (GLASS; November 2018–2022), an unpaid member of the WHO Guidelines Development Group on the treatment of Ebola (2021–23), a paid scientific advisor on COVID-19 immunology to the Scottish Parliament (2021–23), an unpaid member of the Variant Technical Group for SARS-CoV-2 (invited as T-cell specialist) for the UK Health Security Agency (2021 to present), and an unpaid member for UK Government (immunologist) on the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG; 2023 to present). N A Feasey reports grants or contracts from the Environmental Surveillance for Vaccine Impact Assessment (2022–25), National Institute for Health and Care Research (NIHR) Global Health Professorship (2022–27), NeoTrack from the Bill & Melinda Gates Foundation (2021–23), Chatinkha Seq from the Bill & Melinda Gates Foundation (2020–22), and as a co-investigator for Strength in Places (UK Research and Innovation; 2020–25). C E Moore reports support for the present manuscript from the Wellcome Trust grant for The Global Research on Antimicrobial Resistance (GRAM) Project (R52354 CN001). A Pollard reports grants or contracts from the Bill & Melinda Gates Foundation, Wellcome, Cepi, UK Medical Research Council, NIHR, Serum Institute of India, AstraZeneca, and European Commission; royalties or licenses from AstraZeneca (as a contributor to intellectual property licensed by Oxford University Innovation to AstraZeneca); consulting fees from Shionogi; leadership or fiduciary roles in board, society, committee or advocacy groups unpaid with the UK Department of Health and Social Care's Joint Committee on Vaccination and Immunisation as the Chair, and as a member of WHO's Strategic Advisory Group of Experts on Immunization until 2022. J L Walson reports grants from the Bill & Melinda Gates Foundation to support AMR research in Africa. All other authors declare no competing interests.
Figures
Comment in
-
Bacterial antimicrobial resistance burden in Africa: accuracy, action, and alternatives.Lancet Glob Health. 2024 Feb;12(2):e171-e172. doi: 10.1016/S2214-109X(23)00587-9. Epub 2023 Dec 19. Lancet Glob Health. 2024. PMID: 38134945 No abstract available.
References
-
- Sharma A, Singh A, Dar MA, et al. Menace of antimicrobial resistance in LMICs: current surveillance practices and control measures to tackle hostility. J Infect Public Health. 2022;15:172–181. - PubMed
-
- Godman B, Egwuenu A, Wesangula E, et al. Tackling antimicrobial resistance across sub-Saharan Africa: current challenges and implications for the future. Expert Opin Drug Saf. 2022;21:1089–1111. - PubMed
-
- Ndihokubwayo JB, Yahaya AA, Desta AT, et al. Antimicrobial resistance in the African Region: issues, challenges and actions proposed. Afr Health Monit. 2013;16:27–30.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
