

Developing an electronic health record measure of low-value esophagogastroduodenoscopy for GERD at a large academic health system
- PMID: 38135304
- PMCID: PMC10749030
- DOI: 10.1136/bmjoq-2023-002363
Developing an electronic health record measure of low-value esophagogastroduodenoscopy for GERD at a large academic health system
Abstract
Objectives: Low-value esophagogastroduodenoscopies (EGDs) for uncomplicated gastro-oesophageal reflux disease (GERD) can harm patients and raise patient and payer costs. We developed an electronic health record (EHR) 'eMeasure' to detect low-value EGDs.
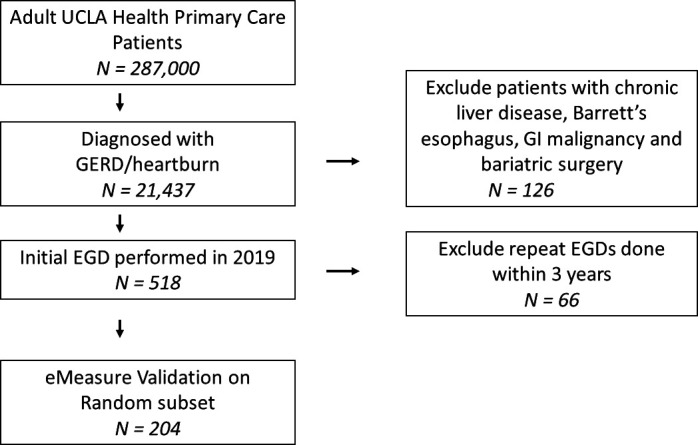
Design: Retrospective cohort of 518 adult patients diagnosed with GERD who underwent initial EGD between 1 January 2019 and 31 December 2019.
Setting: Outpatient primary care and gastroenterology clinics at a large, urban, academic health centre.
Participants: Adult primary care patients at the University of California Los Angeles who underwent initial EGD for GERD in 2019.
Main outcome measures: EGD appropriateness criteria were based on the American College of Gastroenterology 2012 guidelines. An initial EGD was considered low-value if it lacked a documented guideline-based indication, including alarm symptoms (eg, iron-deficiency anaemia); failure of an 8-week proton pump inhibitor trial or elevated Barrett's oesophagus risk. We performed manual chart review on a random sample of 204 patients as a gold standard of the eMeasure's validity. We estimated EGD costs using Medicare physician and facility fee rates.
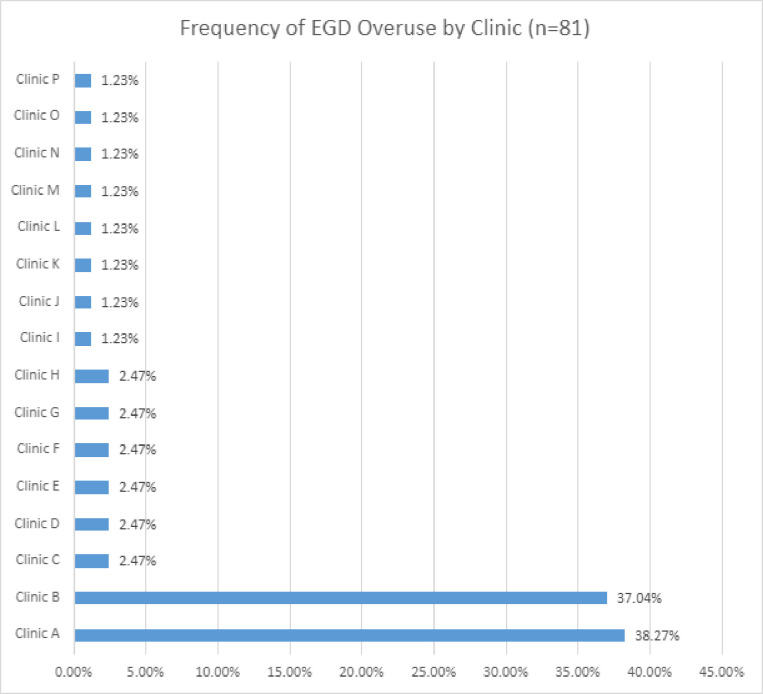
Results: Among 518 initial EGDs performed (mean age 53 years; 54% female), the eMeasure identified 81 (16%) as low-value. The eMeasure's sensitivity was 42% (95% CI 22 to 61) and specificity was 93% (95% CI 89 to 96). Stratifying across clinics, 62 (74.6%) low-value EGDs originated from 2 (12.5%) out of 16 clinics. Total cost for 81 low-value EGDs was approximately US$75 573, including US$14 985 in patients' out-of-pocket costs.
Conclusions: We developed a highly specific eMeasure that showed that low-value EGDs occurred frequently in our healthcare system and were concentrated in a minority of clinics. These results can inform future QI efforts at our institution, such as best practice alerts for the ordering physician. Moreover, this open-source eMeasure has a much broader potential impact, as it can be integrated into any EHR and improve medical decision-making at the point of care.
Keywords: healthcare quality improvement; patient safety; quality improvement.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Dr Mafi reported grants from the National Institute on Aging (NIA) during the conduct of the study, as well as grants from Arnold Ventures and the Commonwealth Fund. Dr. Mafi previously received nonfinancial support from Milliman MedInsight and has provided unpaid consulting to Milliman MedInsight and AHRQ. Ms. Arbanas reported grants from the NIA during the conduct of the study. Dr Sarkisian reported grants from the National Institutes of Health (NIH) during the conduct of the study. No other disclosures were reported.
Figures
Similar articles
-
Low Prevalence of Suspected Barrett's Esophagus in Patients With Gastroesophageal Reflux Disease Without Alarm Symptoms.Clin Gastroenterol Hepatol. 2019 Apr;17(5):857-863. doi: 10.1016/j.cgh.2018.08.066. Epub 2018 Sep 7. Clin Gastroenterol Hepatol. 2019. PMID: 30196157 Free PMC article.
-
Unsedated transnasal ultrathin esophagogastroduodenoscopy may provide better diagnostic performance in gastroesophageal reflux disease.Dis Esophagus. 2011 Feb;24(2):92-8. doi: 10.1111/j.1442-2050.2010.01098.x. Dis Esophagus. 2011. PMID: 20659140
-
Overuse of Repeat Upper Endoscopy in the Veterans Health Administration: A Retrospective Analysis.Am J Gastroenterol. 2017 Nov;112(11):1678-1685. doi: 10.1038/ajg.2017.192. Epub 2017 Jul 11. Am J Gastroenterol. 2017. PMID: 28695907
-
The Second Canadian Consensus Conference on the Management of Patients with Gastroesophageal Reflux Disease.Can J Gastroenterol. 1997 Sep;11 Suppl B:7B-20B. Can J Gastroenterol. 1997. PMID: 9347173 Review.
-
Adequacy of EGD Reporting: a Review of 100 Reports from 100 Endoscopists.J Gastrointest Surg. 2021 May;25(5):1117-1123. doi: 10.1007/s11605-020-04634-2. Epub 2020 Jun 30. J Gastrointest Surg. 2021. PMID: 32607854 Review.