

Para-infectious brain injury in COVID-19 persists at follow-up despite attenuated cytokine and autoantibody responses
- PMID: 38135686
- PMCID: PMC10746705
- DOI: 10.1038/s41467-023-42320-4
Para-infectious brain injury in COVID-19 persists at follow-up despite attenuated cytokine and autoantibody responses
Erratum in
-
Author Correction: Para-infectious brain injury in COVID-19 persists at follow-up despite attenuated cytokine and autoantibody responses.Nat Commun. 2024 Apr 4;15(1):2918. doi: 10.1038/s41467-024-47320-6. Nat Commun. 2024. PMID: 38575615 Free PMC article. No abstract available.
Abstract
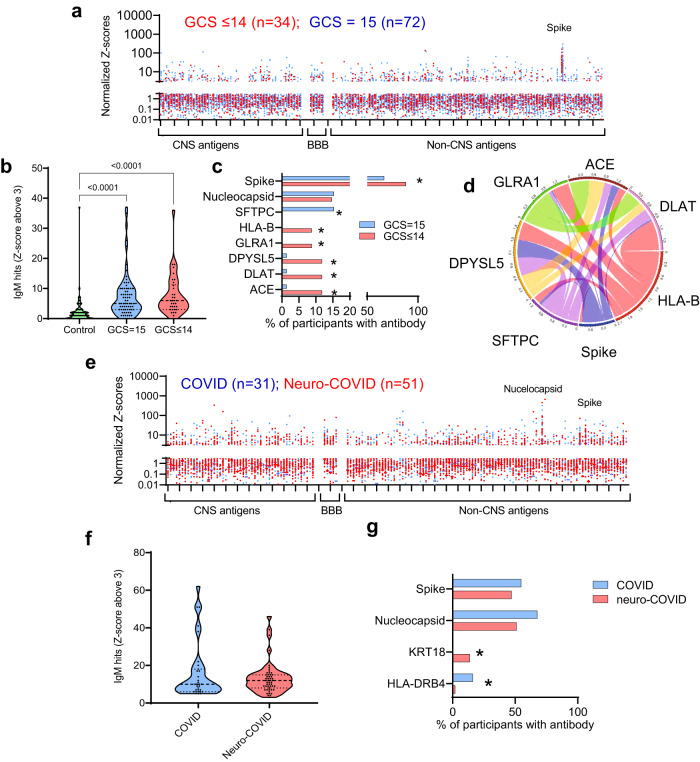
To understand neurological complications of COVID-19 better both acutely and for recovery, we measured markers of brain injury, inflammatory mediators, and autoantibodies in 203 hospitalised participants; 111 with acute sera (1-11 days post-admission) and 92 convalescent sera (56 with COVID-19-associated neurological diagnoses). Here we show that compared to 60 uninfected controls, tTau, GFAP, NfL, and UCH-L1 are increased with COVID-19 infection at acute timepoints and NfL and GFAP are significantly higher in participants with neurological complications. Inflammatory mediators (IL-6, IL-12p40, HGF, M-CSF, CCL2, and IL-1RA) are associated with both altered consciousness and markers of brain injury. Autoantibodies are more common in COVID-19 than controls and some (including against MYL7, UCH-L1, and GRIN3B) are more frequent with altered consciousness. Additionally, convalescent participants with neurological complications show elevated GFAP and NfL, unrelated to attenuated systemic inflammatory mediators and to autoantibody responses. Overall, neurological complications of COVID-19 are associated with evidence of neuroglial injury in both acute and late disease and these correlate with dysregulated innate and adaptive immune responses acutely.
© 2023. The Author(s).
Conflict of interest statement
T.S. is the Director of The Pandemic Institute which has received funding from Innova and CSL Seqirus and Aviva and DAM Health. T.S. was an advisor to the GSK Ebola Vaccine programme and the Siemens Diagnostic Programme. T.S. Chaired the Siemens Healthineers Clinical Advisory Board. T.S. Co-Chaired the WHO Neuro-COVID task force and sat on the UK Government Advisory Committee on Dangerous Pathogens, and the Medicines and Healthcare Products Regulatory Agency (MHRA) Expert Working Group on Covid-19 vaccines. T.S. Advised to the UK COVID-19 Therapeutics Advisory Panel (UK-TAP). T.S. was a Member of COVID-19 Vaccines Benefit Risk Expert Working Group for the Commission on Human Medicines (CHM) committee of the Medicines and Healthcare products Regulatory Agency (MHRA). T.S. has been a member of the Encephalitis Society since 1998 and President of the Encephalitis Society since 2019.
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
