

Breathing Practices for Stress and Anxiety Reduction: Conceptual Framework of Implementation Guidelines Based on a Systematic Review of the Published Literature
- PMID: 38137060
- PMCID: PMC10741869
- DOI: 10.3390/brainsci13121612
Breathing Practices for Stress and Anxiety Reduction: Conceptual Framework of Implementation Guidelines Based on a Systematic Review of the Published Literature
Abstract
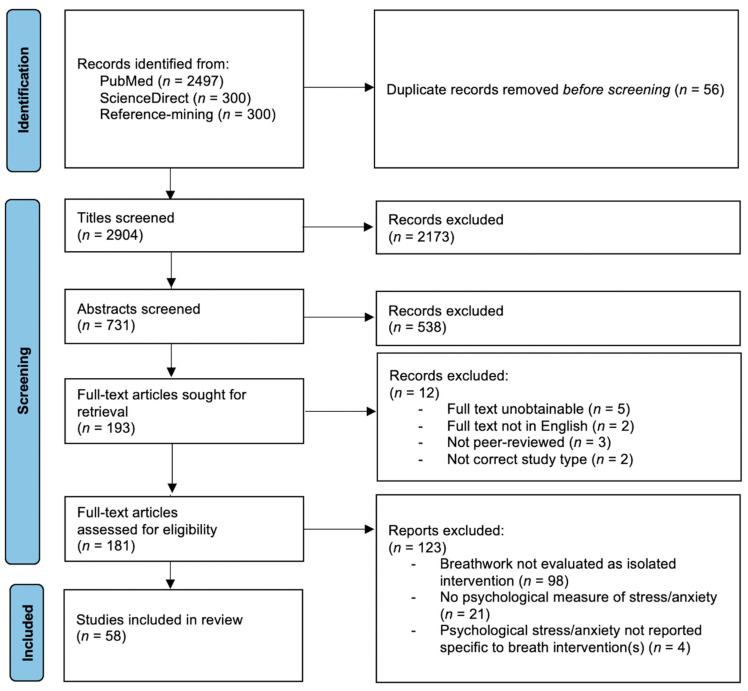
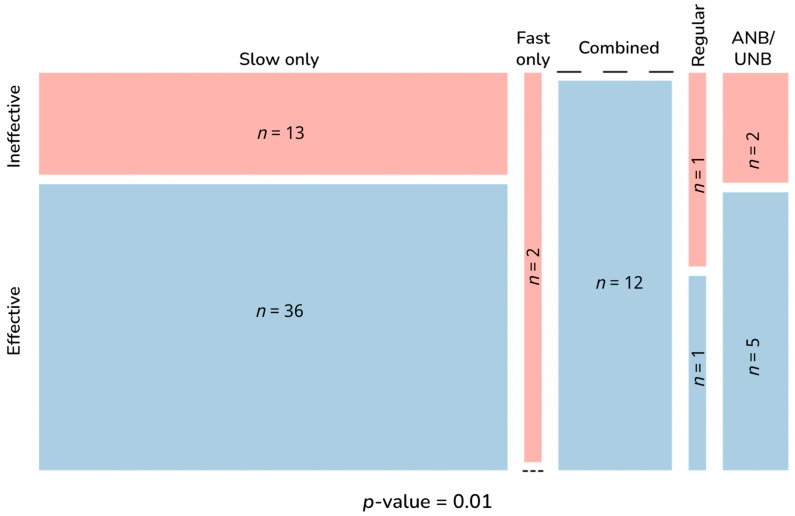
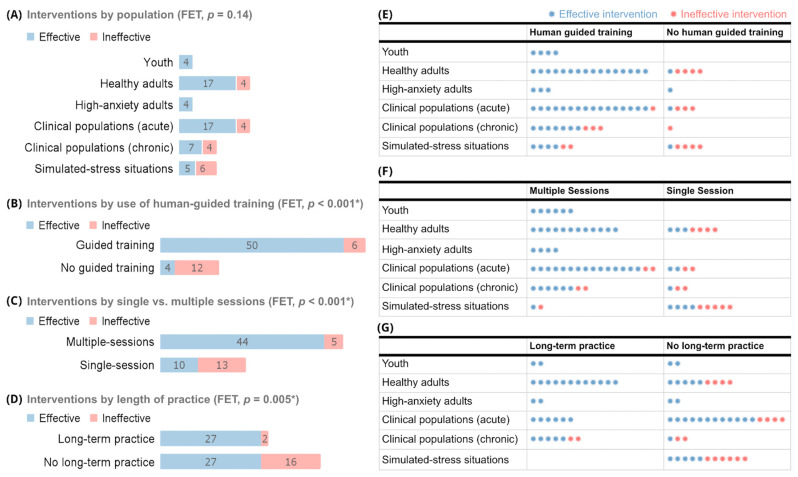
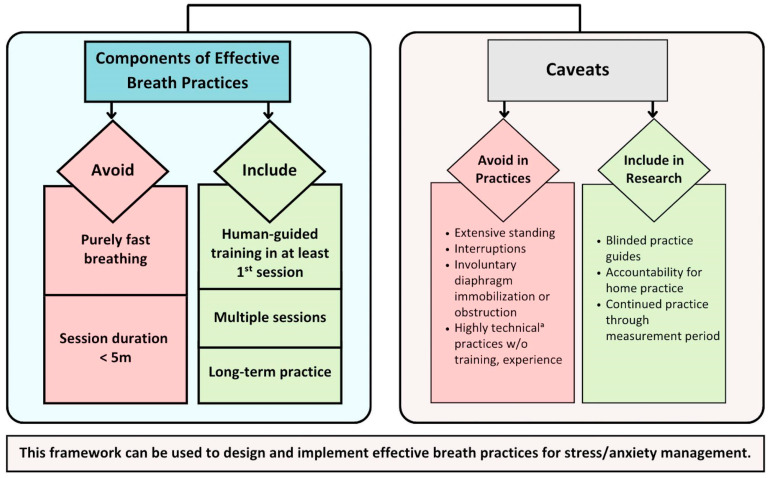
Anxiety and stress plague populations worldwide. Voluntary regulated breathing practices offer a tool to address this epidemic. We examined peer-reviewed published literature to understand effective approaches to and implementation of these practices. PubMed and ScienceDirect were searched to identify clinical trials evaluating isolated breathing-based interventions with psychometric stress/anxiety outcomes. Two independent reviewers conducted all screening and data extraction. Of 2904 unique articles, 731 abstracts, and 181 full texts screened, 58 met the inclusion criteria. Fifty-four of the studies' 72 interventions were effective. Components of effective and ineffective interventions were evaluated to develop a conceptual framework of factors associated with stress/anxiety reduction effectiveness. Effective breath practices avoided fast-only breath paces and sessions <5 min, while including human-guided training, multiple sessions, and long-term practice. Population, other breath paces, session duration ≥5 min, and group versus individual or at-home practices were not associated with effectiveness. Analysis of interventions that did not fit this framework revealed that extensive standing, interruptions, involuntary diaphragmatic obstruction, and inadequate training for highly technical practices may render otherwise promising interventions ineffective. Following this evidence-based framework can help maximize the stress/anxiety reduction benefits of breathing practices. Future research is warranted to further refine this easily accessible intervention for stress/anxiety relief.
Keywords: anxiety; breathing; breathwork; diaphragmatic; pranayama; respiration; stress.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Santomauro D.F., Herrera A.M.M., Shadid J., Zheng P., Ashbaugh C., Pigott D.M., Abbafati C., Adolph C., Amlag J.O., Aravkin A.Y., et al. Global Prevalence and Burden of Depressive and Anxiety Disorders in 204 Countries and Territories in 2020 Due to the COVID-19 Pandemic. Lancet. 2021;398:1700–1712. doi: 10.1016/S0140-6736(21)02143-7. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
