

Exploring the Relationship between Plasma Adiponectin, Gender, and Underlying Diseases in Severe Illness
- PMID: 38137508
- PMCID: PMC10741480
- DOI: 10.3390/biomedicines11123287
Exploring the Relationship between Plasma Adiponectin, Gender, and Underlying Diseases in Severe Illness
Abstract
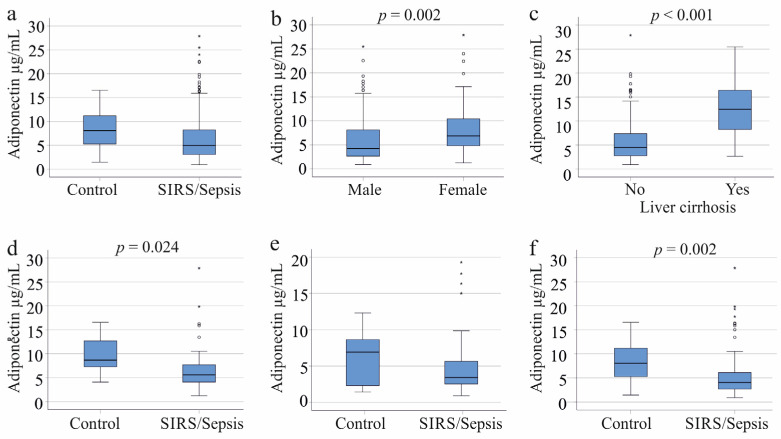
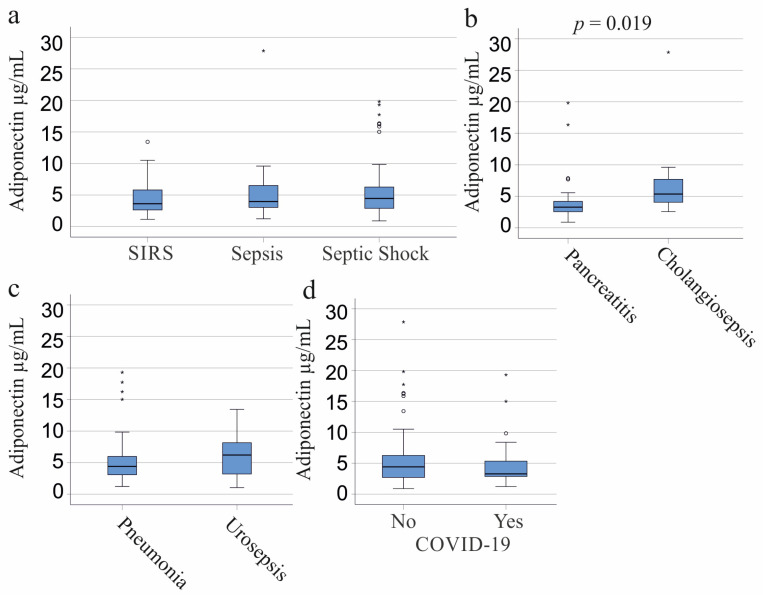
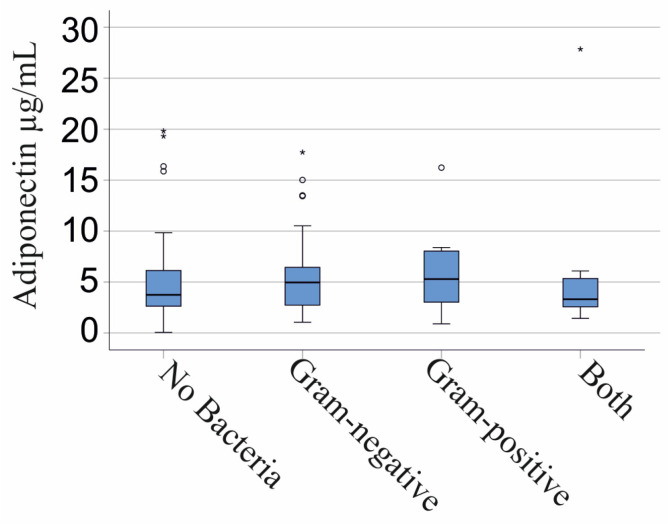
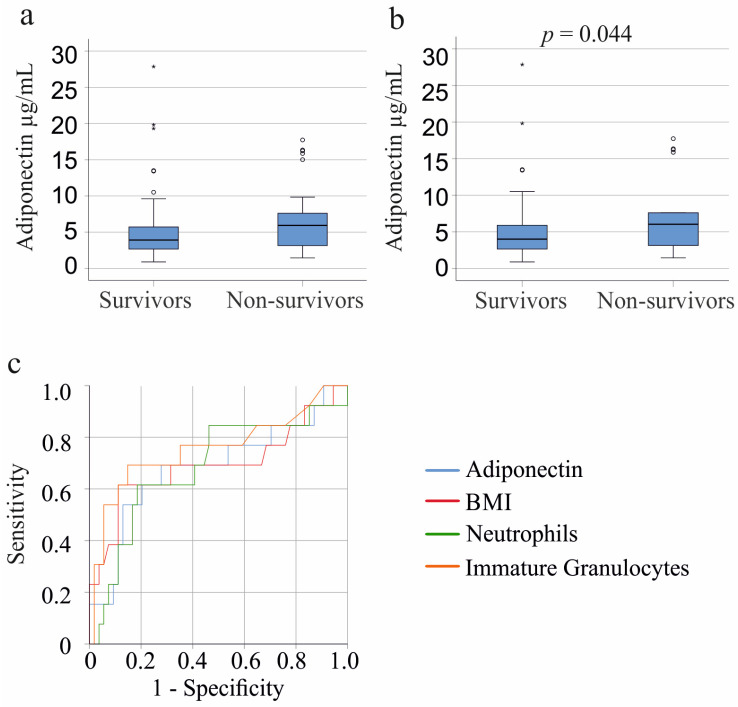
Adiponectin is low in obesity, plays a crucial role in metabolic health, and, moreover, possesses immunoregulatory properties. However, studies examining its levels in patients with systemic inflammatory response syndrome (SIRS) or sepsis have yielded conflicting results. While females typically have higher systemic adiponectin levels than males, research on sex-specific associations in this context is limited. In this study of 156 SIRS/sepsis patients, including those with liver cirrhosis, we aimed to explore the relationship between plasma adiponectin, body mass index (BMI), gender, disease severity, and underlying etiological conditions. Our findings revealed that patients with liver cirrhosis, who are susceptible to infections, exhibited elevated circulating adiponectin levels, irrespective of sex. When excluding cirrhosis patients, plasma adiponectin levels were similar between male SIRS/sepsis patients and controls but lower in female patients compared to female controls. Plasma adiponectin was inversely related to BMI in female but not male patients. Further analysis within the non-cirrhosis subgroup demonstrated no significant differences in adiponectin levels between sexes among SIRS, sepsis, and septic shock patients. Ventilation, dialysis, and vasopressor therapy had no discernible impact on adiponectin levels in either sex. A negative correlation between adiponectin and C-reactive protein (CRP) existed in males only. Notably, patients with pancreatitis showed the lowest plasma adiponectin concentrations, although sex-specific differences were not significant. Infection with Gram-negative or Gram-positive bacteria had minimal effects on plasma adiponectin levels in both sexes. However, infection with the severe acute respiratory syndrome coronavirus type 2 led to decreased adiponectin levels in females exclusively. Multivariate analysis considering all factors affecting plasma adiponectin levels in males or females identified BMI in females and CRP levels in males to predict plasma adiponectin levels in SIRS/sepsis patients. Additionally, our study observed a trend where the 25 patients who did not survive had higher plasma adiponectin levels, particularly among males. In summary, our investigation highlights the influence of underlying diseases and sex on plasma adiponectin levels in SIRS/sepsis patients, shedding light on potential implications for disease management and prognosis.
Keywords: COVID-19; adiponectin; liver cirrhosis; pancreatitis; sex; survival.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ikeagwulonu R.C., Ugwu N.I., Ezeonu C.T., Ikeagwulonu Z.C., Uro-Chukwu H.C., Asiegbu U.V., Obu D.C., Briggs D.C. C-Reactive Protein and COVID-19 Severity: A Systematic Review. West. Afr. J. Med. 2021;38:1011–1023. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
