

When Atrial Fibrillation Meets Cerebral Amyloid Angiopathy: Current Evidence and Strategies
- PMID: 38137773
- PMCID: PMC10743760
- DOI: 10.3390/jcm12247704
When Atrial Fibrillation Meets Cerebral Amyloid Angiopathy: Current Evidence and Strategies
Abstract
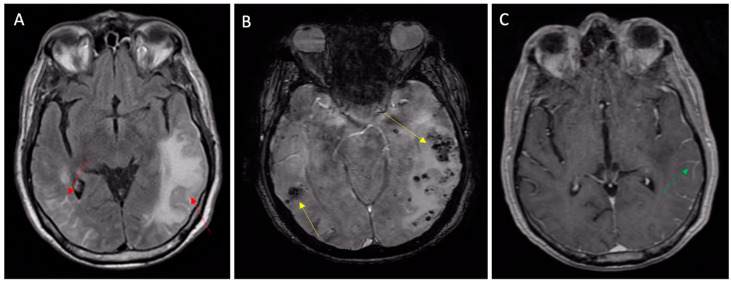
Non-valvular atrial fibrillation (AF) and cerebral amyloid angiopathy (CAA) are two common diseases in elderly populations. Despite the effectiveness of oral anticoagulant therapy in cardioembolic stroke prevention, intracranial hemorrhage represents the most serious complication of these therapies. Cerebral amyloid angiopathy is one of the main risk factors for spontaneous intracranial bleeding, and this risk is highly increased by age and concomitant antithrombotic therapies. Cerebral amyloid angiopathy can be silent for years and then manifest with clinical features simulating TIA (TIA-mimics) or stroke in AF patients, pushing clinicians to rapidly start VKAs or DOACs, thus increasing the risk of intracranial bleeding if the diagnosis of CAA was unknown. Because the cerebral amyloid angiopathy is easily diagnosed with non-contrast MRI, suspecting the disease can avoid catastrophic complications. In this review, we will provide physicians managing anticoagulant therapies with key tips to familiarize themselves with cerebral amyloid angiopathy, with a focus on the possible clinical presentations and on the diagnostic criteria.
Keywords: anticoagulation; atrial fibrillation; cerebral amyloid angiopathy; high bleeding risk; intracranial hemorrhage; left-atrial appendage occlusion.
Conflict of interest statement
We declare that we have no conflict of interest.
Figures



References
-
- Miyasaka Y., Barnes M.E., Gersh B.J., Cha S.S., Bailey K.R., Abhayaratna W.P., Seward J.B., Tsang T.S. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation. 2006;114:119–125. doi: 10.1161/CIRCULATIONAHA.105.595140. - DOI - PubMed
-
- Hindricks G., Potpara T., Dagres N., Arbelo E., Bax J.J., Blomström-Lundqvist C., Boriani G., Castella M., Dan G.-A., Dilaveris P.E., et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021;42:373–498. doi: 10.1093/eurheartj/ehaa612. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
