

The Rate of Postoperative Complications in Complicated Acute, and Subacute Type B Aortic Dissections after TEVAR vs. PETTICOAT Procedures: Systematic Review and Meta-Analysis
- PMID: 38138253
- PMCID: PMC10744781
- DOI: 10.3390/medicina59122150
The Rate of Postoperative Complications in Complicated Acute, and Subacute Type B Aortic Dissections after TEVAR vs. PETTICOAT Procedures: Systematic Review and Meta-Analysis
Abstract
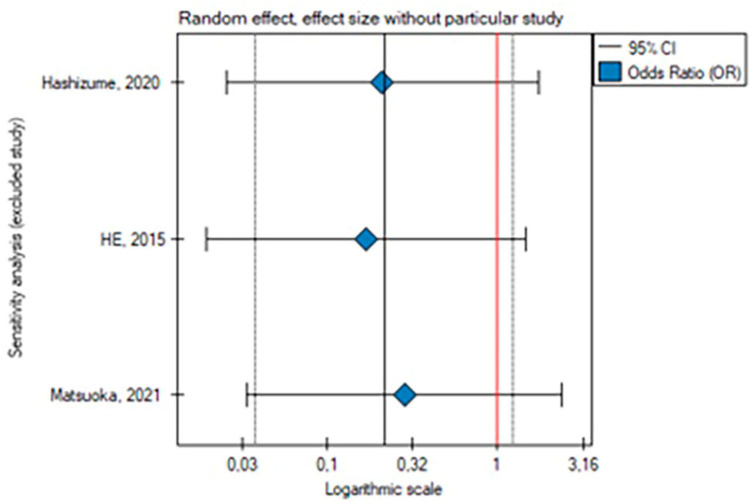
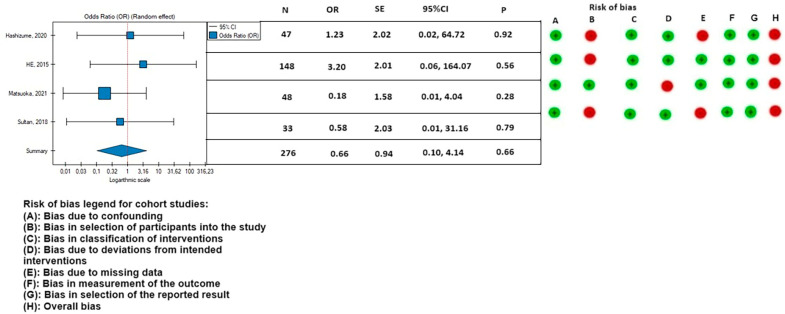
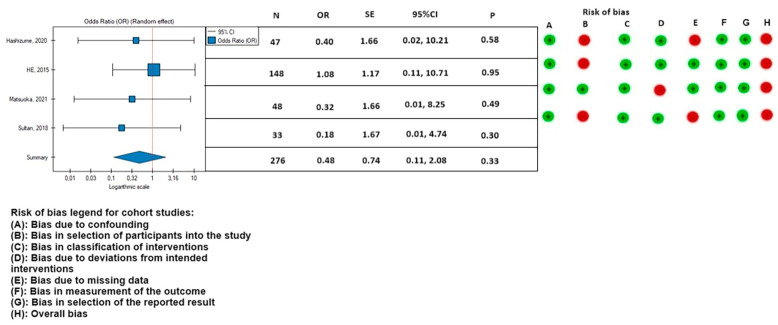
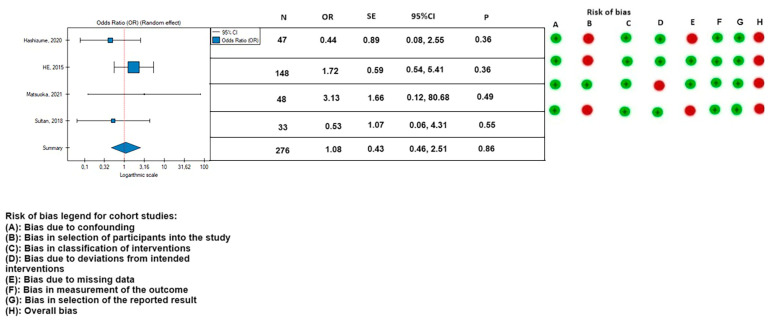
Background and Objectives: Provisional extension to induce complete attachment (PETTICOAT) is suggested as being associated with a lower incidence of aorta-related events and fewer reinterventions compared to thoracic endovascular aortic repair (TEVAR) in patients with complicated acute, and subacute type B aortic dissections. Materials and Methods: This article is a systematic review and meta-analysis following the PRISMA guidelines. The Medline, PubMed, Embase, and Cochrane databases were searched, starting on 21 February 2022 and ending on 22 June 2022, to identify studies that investigated the rate of postoperative complications in patients treated with the PETTICOAT compared to the TEVAR. A random effects meta-analysis was performed. Of 2350 studies, 5 studies involving 360 patients were included: 143 patients after the PETTICOAT procedure and 217 after the TEVAR. Results: The meta-analysis of all studies showed that the rate of secondary endovascular reinterventions was smaller in patients treated with the PETTICOAT (n = 3 studies; OR, 0.30; 95% CI, 0.10 to 0.94; p = 0.04). The results of other postoperative complications (30-day mortality, mortality during follow-up, paraplegia, stroke, and occurrence of endoleak) were lower in the PETTICOAT group but were not statistically significant. The rate of postoperative renal failure was lower in patients treated with the TEVAR (n = 4; OR, 1.08; 95% CI, 0.46 to 2.51; p = 0.86). Conclusion: This meta-analysis suggests that the PETTICOAT procedure is related to the lower rate of secondary endovascular reinterventions for complicated acute, and subacute type B aortic dissections.
Keywords: PETTICOAT; TEVAR with bare metal stent; endovascular reinterventions.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







References
-
- Matsuoka T., Hashizume K., Honda M., Harada D., Ohno M., Ikebata K., Kaneyama H., Takaki H., Lefor A.K., Sasaki J., et al. The provisional extension to induce complete attachment technique is associated with abdominal aortic remodeling and reduces aorta-related adverse events after aortic dissection. J. Vasc. Surg. 2021;74:45–52.e1. doi: 10.1016/j.jvs.2020.11.038. - DOI - PubMed
-
- Hashizume K., Honda M., Mori M., Yagami T., Takaki H., Matsuoka T., Ikebata K., Kanayama H., Ohno M., Shimizu H. Full PETTICOAT in acute type B aortic dissection with patent false lumen may offer positive remodeling for the distal aorta. Gen. Thorac. Cardiovasc. Surg. 2021;69:926–933. doi: 10.1007/s11748-020-01548-3. - DOI - PubMed
-
- Molinari A.C., Leo E., Ferraresi M., Ferrari S.A., Terzi A., Sommaruga S., Rossi G. Distal Extended Endovascular Aortic Repair PETTICOAT: A Modified Technique to Improve False Lumen Remodeling in Acute Type B Aortic Dissection. Ann. Vasc. Surg. 2019;59:300–305. doi: 10.1016/j.avsg.2019.02.053. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
