

Non-Invasive Assessment of Abdominal/Diaphragmatic and Thoracic/Intercostal Spontaneous Breathing Contributions
- PMID: 38139620
- PMCID: PMC10747041
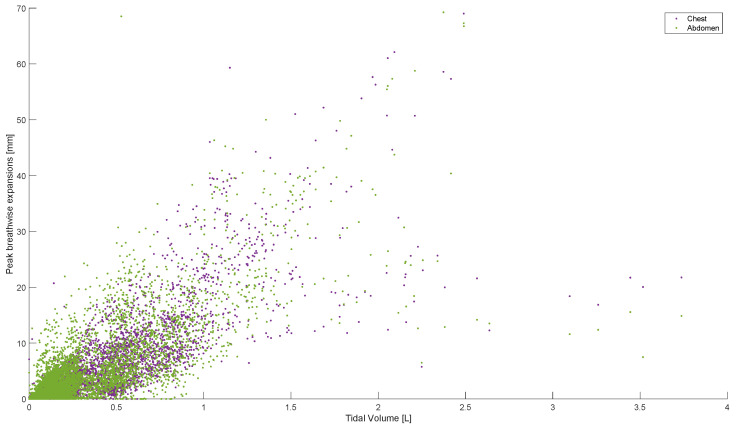
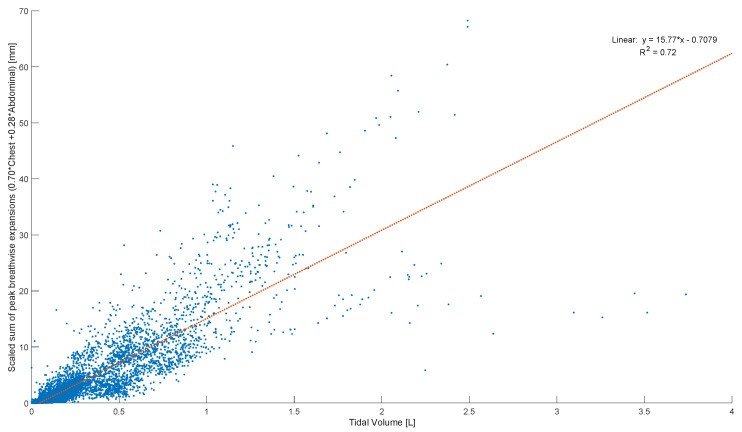
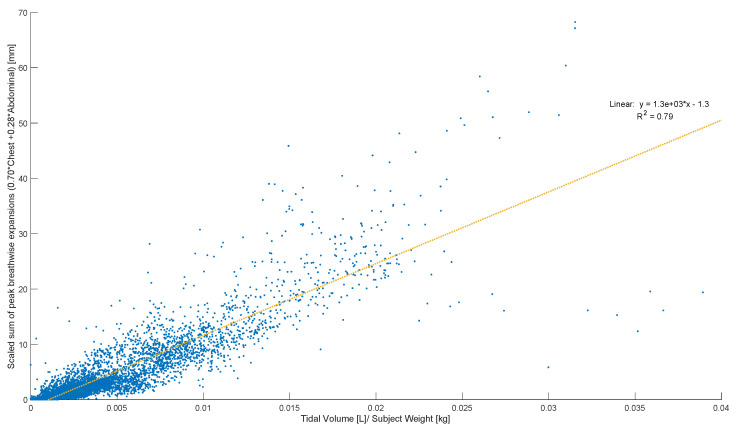
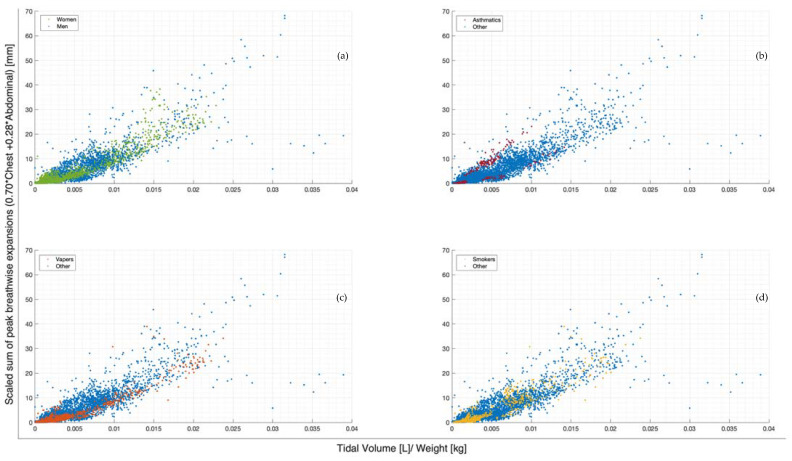
- DOI: 10.3390/s23249774
Non-Invasive Assessment of Abdominal/Diaphragmatic and Thoracic/Intercostal Spontaneous Breathing Contributions
Abstract
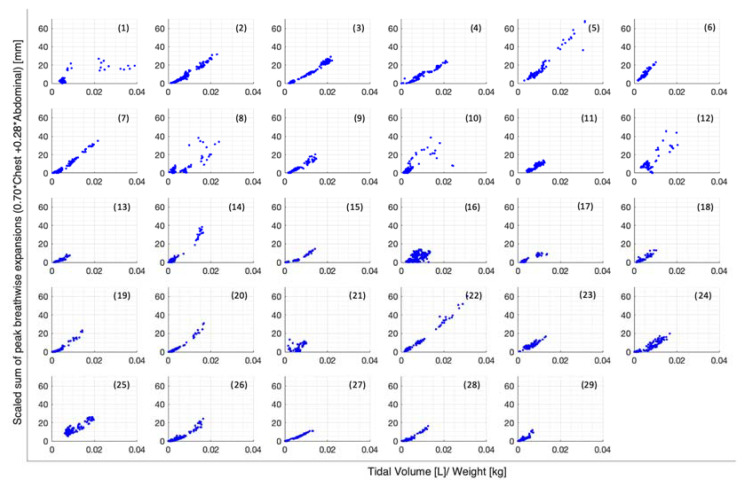
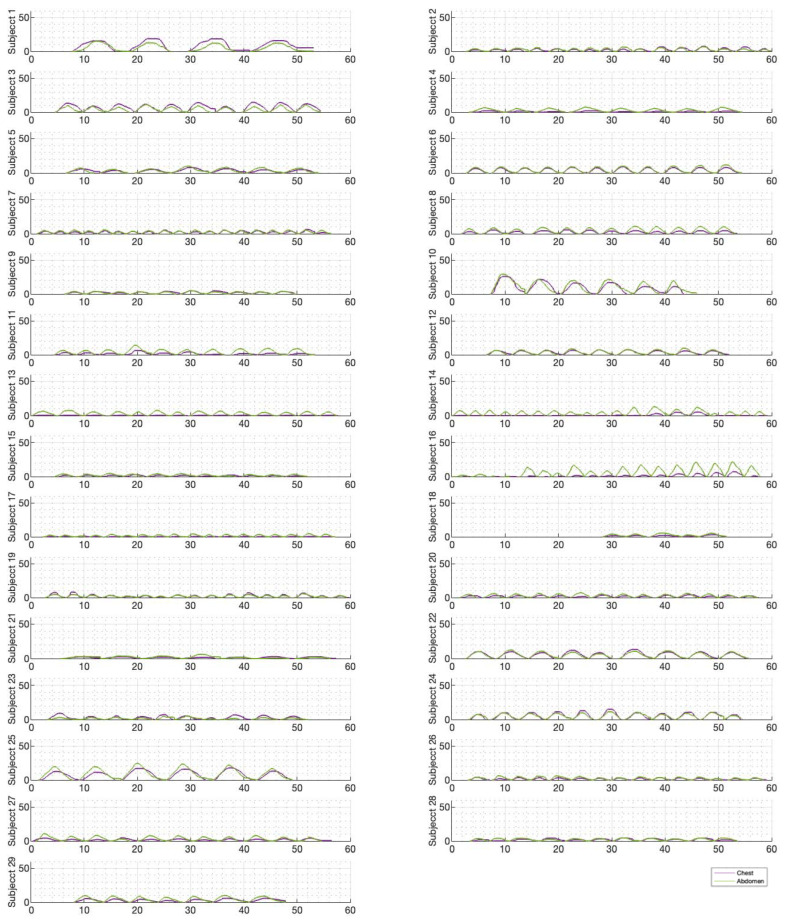
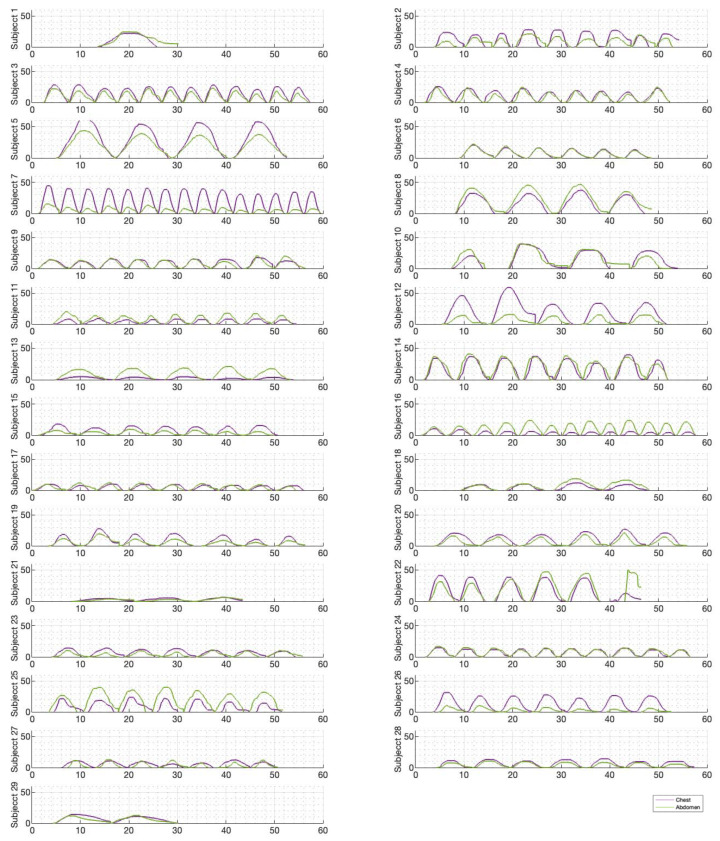
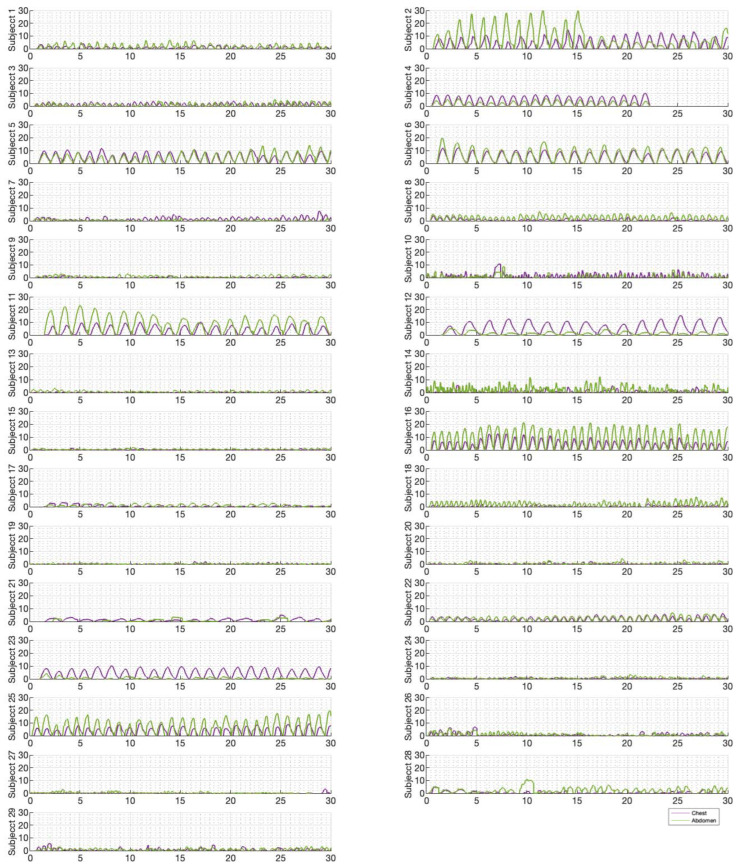
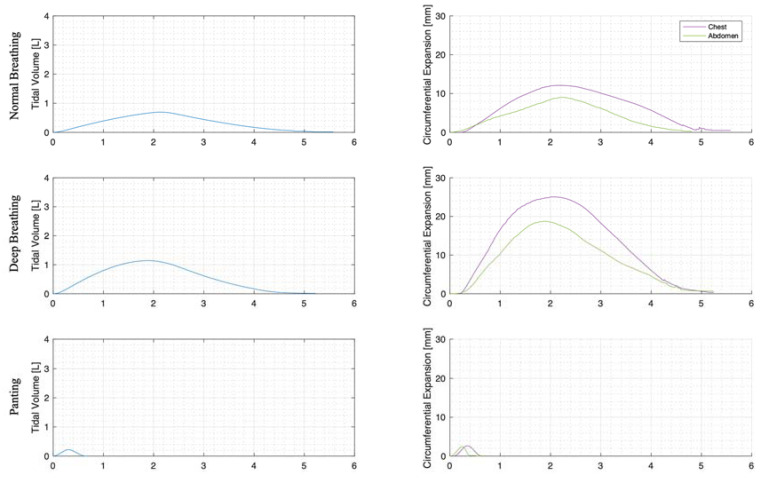
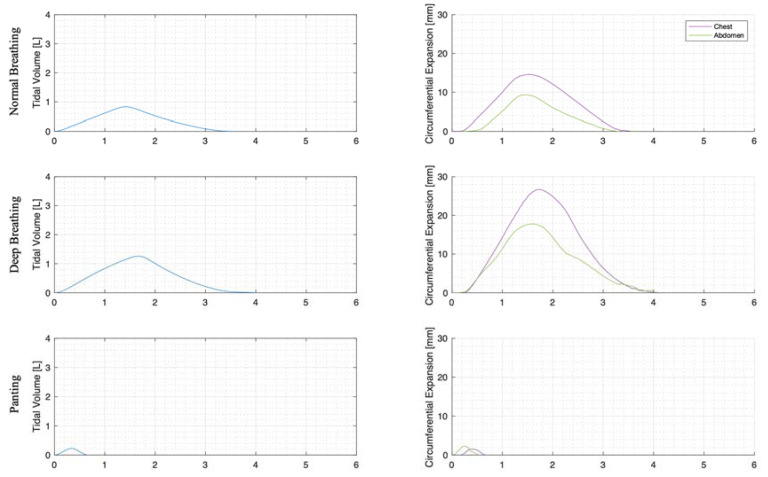
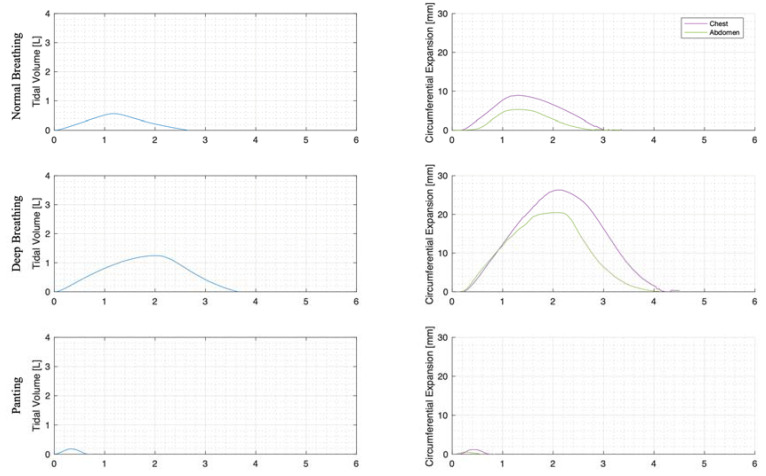
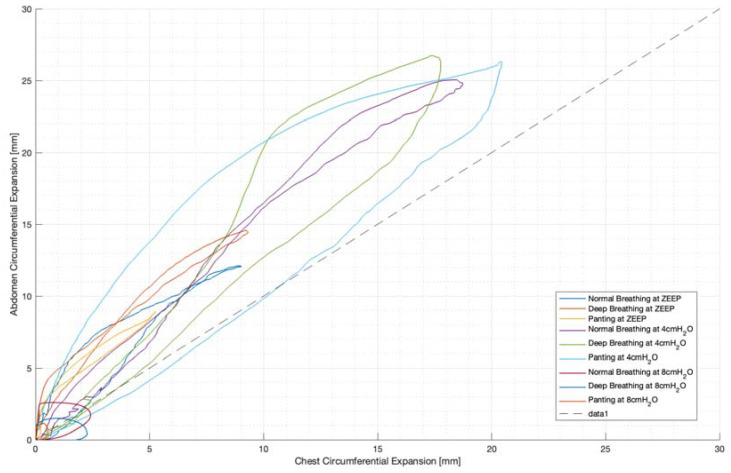
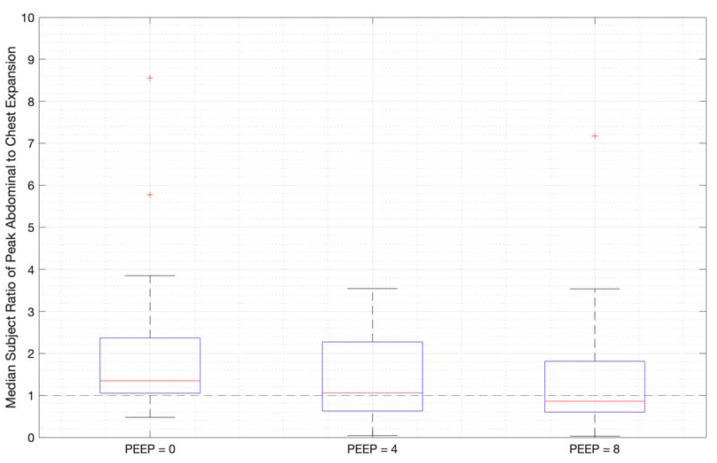
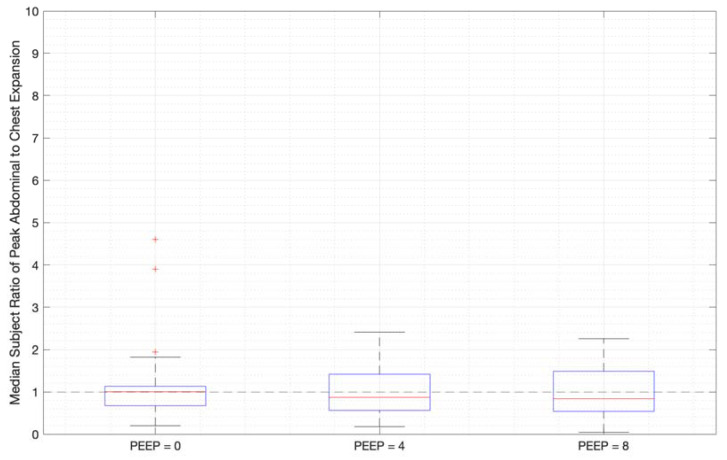
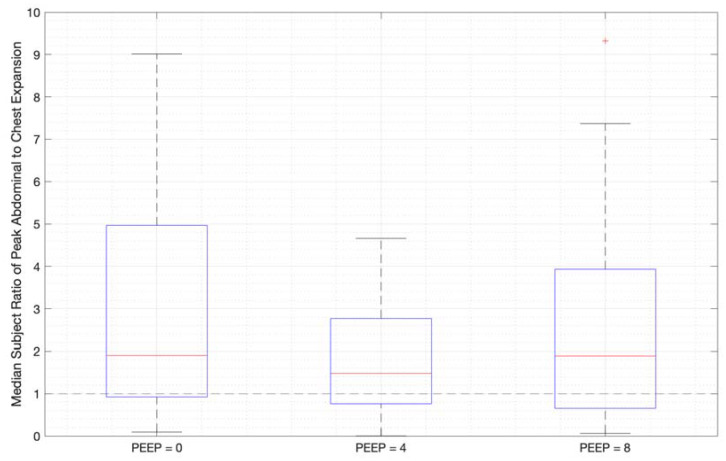
(1) Background: Technically, a simple, inexpensive, and non-invasive method of ascertaining volume changes in thoracic and abdominal cavities are required to expedite the development and validation of pulmonary mechanics models. Clinically, this measure enables the real-time monitoring of muscular recruitment patterns and breathing effort. Thus, it has the potential, for example, to help differentiate between respiratory disease and dysfunctional breathing, which otherwise can present with similar symptoms such as breath rate. Current automatic methods of measuring chest expansion are invasive, intrusive, and/or difficult to conduct in conjunction with pulmonary function testing (spontaneous breathing pressure and flow measurements). (2) Methods: A tape measure and rotary encoder band system developed by the authors was used to directly measure changes in thoracic and abdominal circumferences without the calibration required for analogous strain-gauge-based or image processing solutions. (3) Results: Using scaling factors from the literature allowed for the conversion of thoracic and abdominal motion to lung volume, combining motion measurements correlated to flow-based measured tidal volume (normalised by subject weight) with R2 = 0.79 in data from 29 healthy adult subjects during panting, normal, and deep breathing at 0 cmH2O (ZEEP), 4 cmH2O, and 8 cmH2O PEEP (positive end-expiratory pressure). However, the correlation for individual subjects is substantially higher, indicating size and other physiological differences should be accounted for in scaling. The pattern of abdominal and chest expansion was captured, allowing for the analysis of muscular recruitment patterns over different breathing modes and the differentiation of active and passive modes. (4) Conclusions: The method and measuring device(s) enable the validation of patient-specific lung mechanics models and accurately elucidate diaphragmatic-driven volume changes due to intercostal/chest-wall muscular recruitment and elastic recoil.
Keywords: abdominal; circumference; monitoring; muscular recruitment; respiratory mechanics; rotary encoder; thoracic.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
[Standard technical specifications for methacholine chloride (Methacholine) bronchial challenge test (2023)].Zhonghua Jie He He Hu Xi Za Zhi. 2024 Feb 12;47(2):101-119. doi: 10.3760/cma.j.cn112147-20231019-00247. Zhonghua Jie He He Hu Xi Za Zhi. 2024. PMID: 38309959 Chinese.
-
Adaptation of lung, chest wall, and respiratory muscles during pregnancy: preparing for birth.J Appl Physiol (1985). 2019 Dec 1;127(6):1640-1650. doi: 10.1152/japplphysiol.00035.2019. Epub 2019 Nov 7. J Appl Physiol (1985). 2019. PMID: 31697596
-
Chest wall mechanics during pressure support ventilation.Crit Care. 2006;10(2):R54. doi: 10.1186/cc4867. Crit Care. 2006. PMID: 16584534 Free PMC article.
-
Can diaphragmatic breathing modify chest wall volumes during inspiratory loaded breathing in patients with heart failure?Braz J Phys Ther. 2018 Nov-Dec;22(6):452-458. doi: 10.1016/j.bjpt.2018.04.005. Epub 2018 Apr 17. Braz J Phys Ther. 2018. PMID: 29752160 Free PMC article.
-
Options for assessing and measuring chest wall motion.Paediatr Respir Rev. 2015 Jan;16(1):3-10. doi: 10.1016/j.prrv.2014.10.006. Epub 2014 Oct 29. Paediatr Respir Rev. 2015. PMID: 25468220 Review.
Cited by
-
Symptoms Arising From the Diaphragm Muscle: Function and Dysfunction.Cureus. 2024 Jan 29;16(1):e53143. doi: 10.7759/cureus.53143. eCollection 2024 Jan. Cureus. 2024. PMID: 38288323 Free PMC article. Review.
-
Pulmonary function testing dataset of pressure and flow, dynamic circumference, heart rate, and aeration monitoring.Data Brief. 2024 Apr 4;54:110386. doi: 10.1016/j.dib.2024.110386. eCollection 2024 Jun. Data Brief. 2024. PMID: 38646196 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
