

Accurate prediction of biliary atresia with an integrated model using MMP-7 levels and bile acids
- PMID: 38141111
- PMCID: PMC11402860
- DOI: 10.1007/s12519-023-00779-7
Accurate prediction of biliary atresia with an integrated model using MMP-7 levels and bile acids
Abstract
Background: Biliary atresia (BA) is a rare fatal liver disease in children, and the aim of this study was to develop a method to diagnose BA early.
Methods: We determined serum levels of matrix metalloproteinase-7 (MMP-7), the results of 13 liver tests, and the levels of 20 bile acids, and integrated computational models were constructed to diagnose BA.
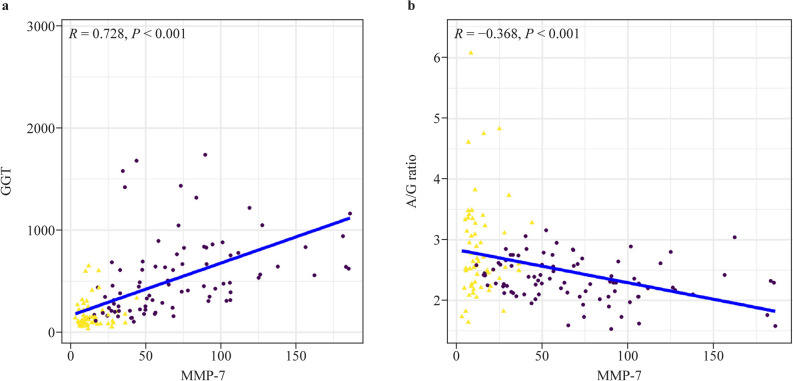
Results: Our findings demonstrated that MMP-7 expression levels, as well as the results of four liver tests and levels of ten bile acids, were significantly different between 86 BA and 59 non-BA patients (P < 0.05). The computational prediction model revealed that MMP-7 levels alone had a higher predictive accuracy [area under the receiver operating characteristic curve (AUC) = 0.966, 95% confidence interval (CI): 0.942, 0.989] than liver test results and bile acid levels. The AUC was 0.890 (95% CI 0.837, 0.943) for liver test results and 0.825 (95% CI 0.758, 0.892) for bile acid levels. Furthermore, bile levels had a higher contribution to enhancing the predictive accuracy of MMP-7 levels (AUC = 0.976, 95% CI 0.953, 1.000) than liver test results. The AUC was 0.983 (95% CI 0.962, 1.000) for MMP-7 levels combined with liver test results and bile acid levels. In addition, we found that MMP-7 levels were highly correlated with gamma-glutamyl transferase levels and the liver fibrosis score.
Conclusion: The innovative integrated models based on a large number of indicators provide a noninvasive and cost-effective approach for accurately diagnosing BA in children. Video Abstract (MP4 142103 KB).
Keywords: Bile aid; Biliary atresia; Diagnosis; Liver fibrosis; Liver test; MMP-7.
© 2023. The Author(s).
Conflict of interest statement
No financial or non-financial benefits have been received or will be received from any party related directly or indirectly to the subject of this article. Author Li-Zhong Du is a member of the Editorial Board for
Figures





References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
