

Changes in the global hospitalisation burden of respiratory syncytial virus in young children during the COVID-19 pandemic: a systematic analysis
- PMID: 38141633
- PMCID: PMC11290460
- DOI: 10.1016/S1473-3099(23)00630-8
Changes in the global hospitalisation burden of respiratory syncytial virus in young children during the COVID-19 pandemic: a systematic analysis
Abstract
Background: The COVID-19 pandemic is reported to have affected the epidemiology of respiratory syncytial virus (RSV), which could have important implications for RSV prevention and control strategies. We aimed to assess the hospitalisation burden of RSV-associated acute lower respiratory infection (ALRI) in children younger than 5 years during the pandemic period and the possible changes in RSV epidemiology from a global perspective.
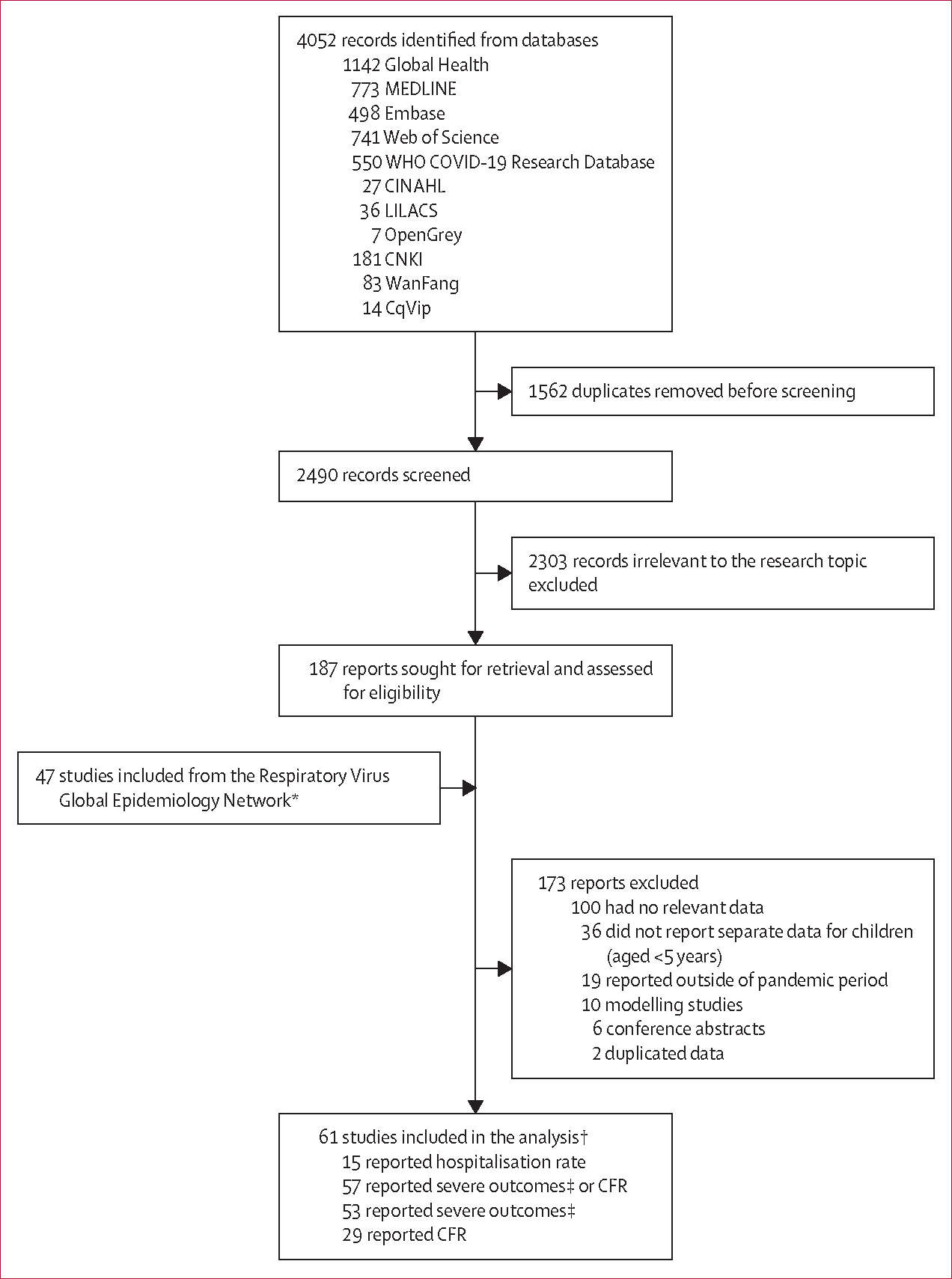
Methods: We conducted a systematic literature search for studies published between Jan 1, 2020, and June 30, 2022, in MEDLINE, Embase, Global Health, Web of Science, the WHO COVID-19 Research Database, CINAHL, LILACS, OpenGrey, CNKI, WanFang, and CqVip. We included unpublished data on RSV epidemiology shared by international collaborators. Eligible studies reported data on at least one of the following measures for children (aged <5 years) hospitalised with RSV-associated ALRI: hospital admission rates, in-hospital case fatality ratio, and the proportion of hospitalised children requiring supplemental oxygen or requiring mechanical ventilation or admission to intensive care. We used a generalised linear mixed-effects model for data synthesis to measure the changes in the incidence, age distribution, and disease severity of children hospitalised with RSV-associated ALRI during the pandemic, compared with the year 2019.
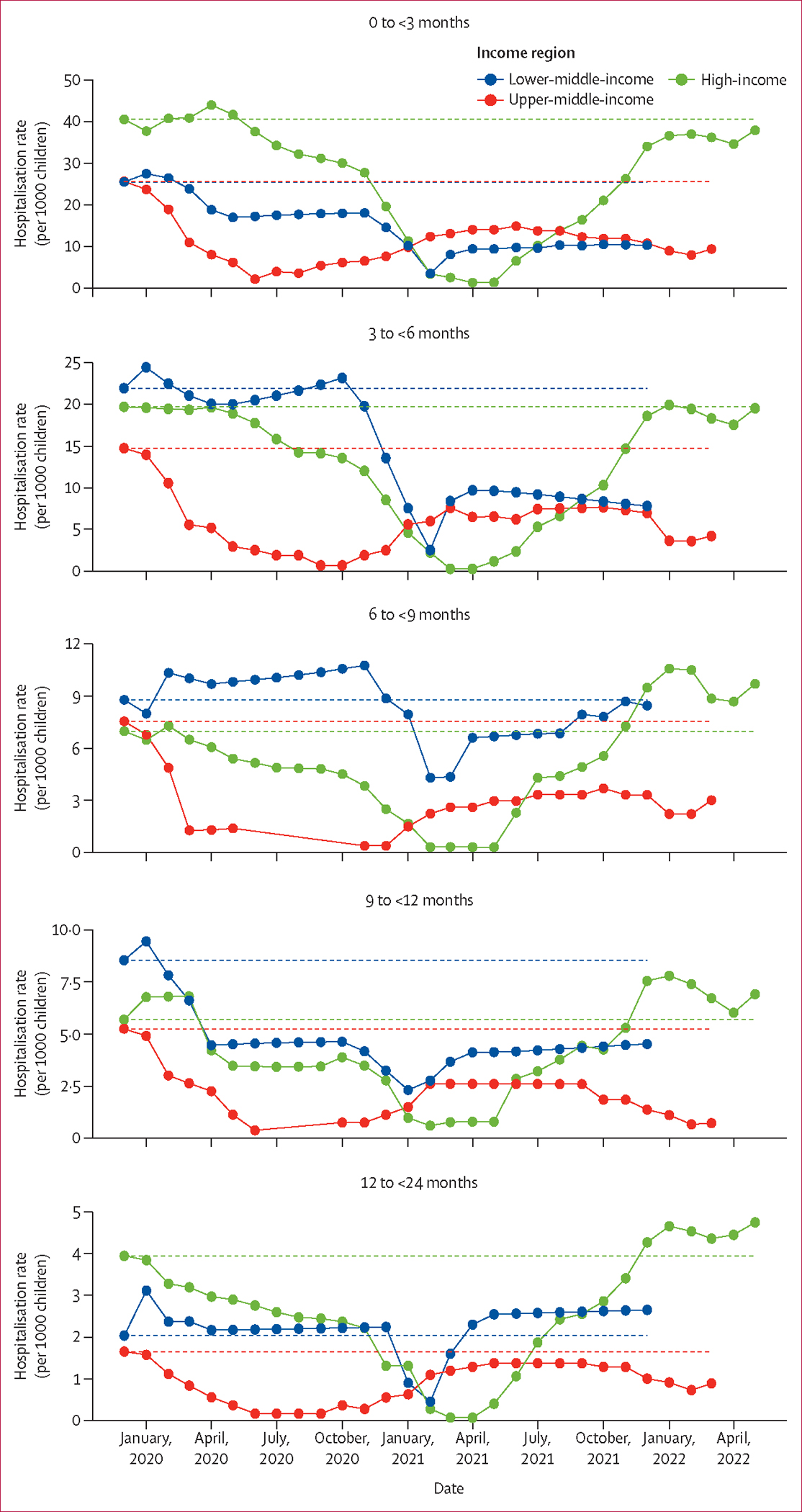
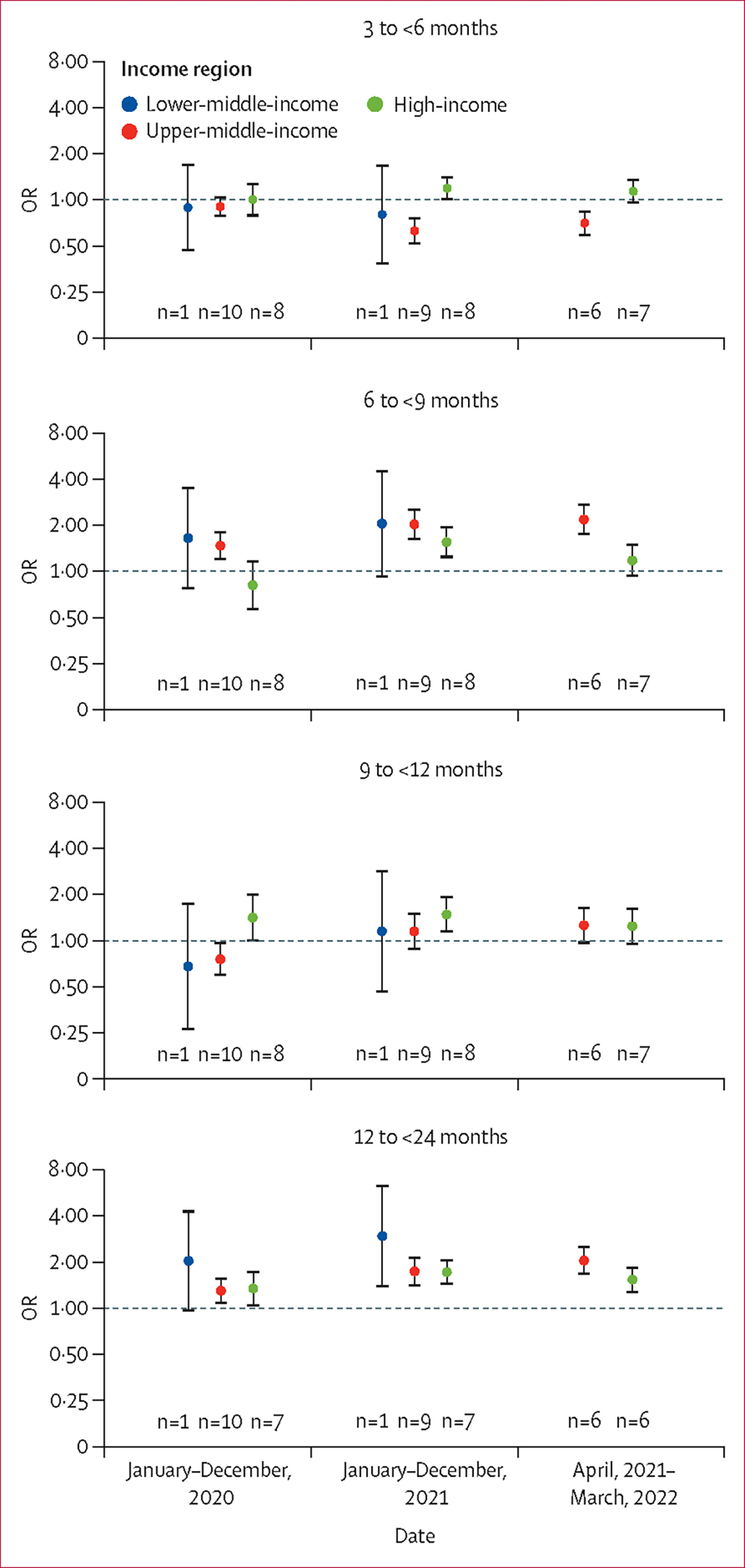
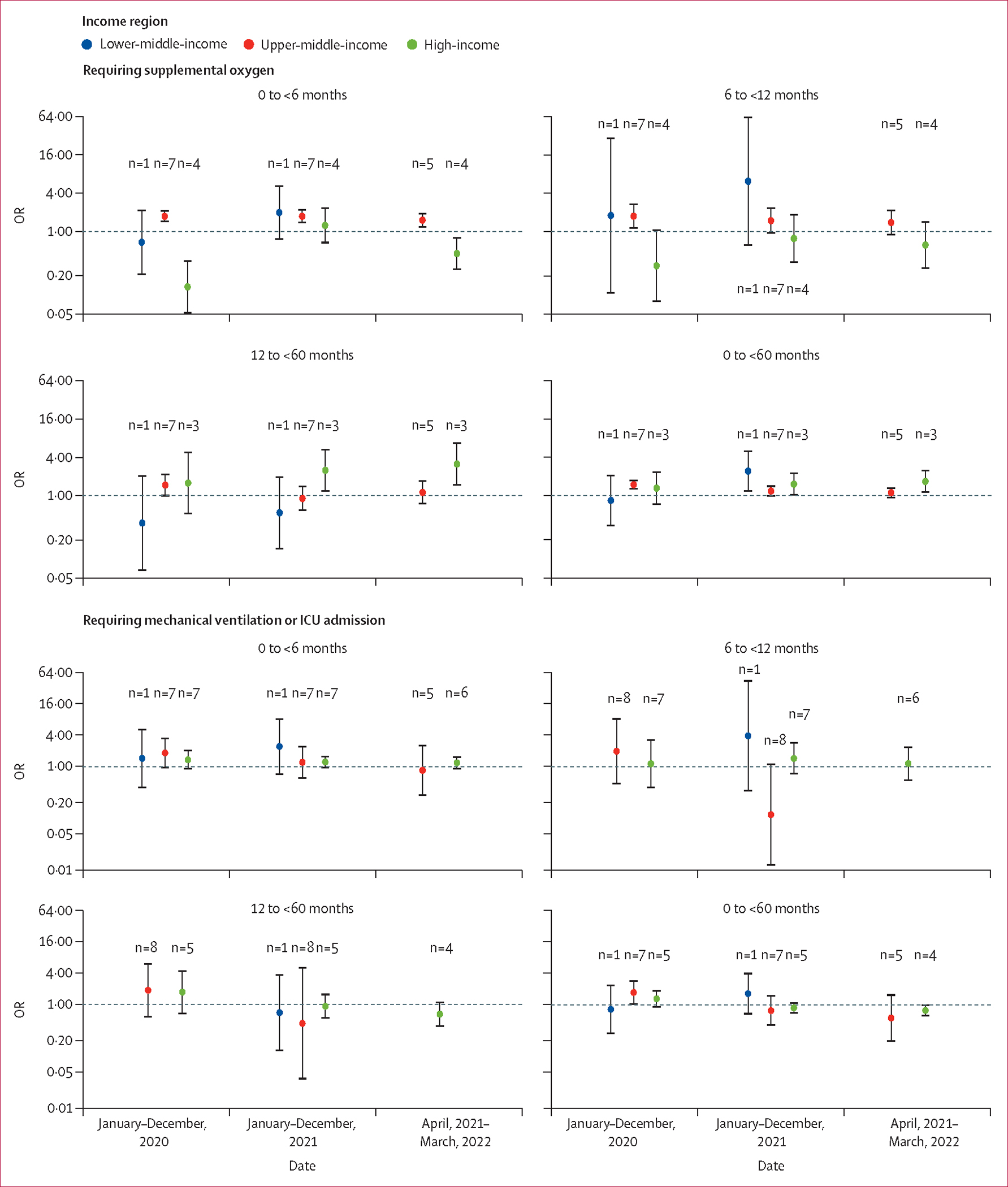
Findings: We included 61 studies from 19 countries, of which 14 (23%) studies were from the published literature (4052 identified records) and 47 (77%) were from unpublished datasets. Most (51 [84%]) studies were from high-income countries; nine (15%) were from upper-middle-income countries, one (2%) was from a lower-middle-income country (Kenya), and none were from a low-income country. 15 studies contributed to the estimates of hospitalisation rate and 57 studies contributed to the severity analyses. Compared with 2019, the rates of RSV-associated ALRI hospitalisation in all children (aged 0-60 months) in 2020 decreased by 79·7% (325 000 cases vs 66 000 cases) in high-income countries, 13·8% (581 000 cases vs 501 000 cases) in upper-middle-income countries, and 42·3% (1 378 000 cases vs 795 000 cases) in Kenya. In high-income countries, annualised rates started to rise in 2021, and by March, 2022, had returned to a level similar to 2019 (6·0 cases per 1000 children [95% uncertainty interval 5·4-6·8] in April, 2021, to March, 2022, vs 5·0 cases per 1000 children [3·6-6·8] in 2019). By contrast, in middle-income countries, rates remained lower in the latest period with data available than in 2019 (for upper-middle-income countries, 2·1 cases [0·7-6·1] in April, 2021, to March, 2022, vs 3·4 [1·2-9·7] in 2019; for Kenya, 2·2 cases [1·8-2·7] in 2021 vs 4·1 [3·5-4·7] in 2019). Across all time periods and income regions, hospitalisation rates peaked in younger infants (aged 0 to <3 months) and decreased with increasing age. A significantly higher proportion of children aged 12-24 months were hospitalised with RSV-associated ALRI in high-income and upper-middle-income countries during the pandemic years than in 2019, with odds ratios ranging from 1·30 (95% uncertainty interval 1·07-1·59) to 2·05 (1·66-2·54). No consistent changes in disease severity were observed.
Interpretation: The hospitalisation burden of RSV-associated ALRI in children younger than 5 years was significantly reduced during the first year of the COVID-19 pandemic. The rebound in hospitalisation rates to pre-pandemic rates observed in the high-income region but not in the middle-income region by March, 2022, suggests a persistent negative impact of the pandemic on health-care systems and health-care access in the middle-income region. RSV surveillance needs to be established (or re-established) to monitor changes in RSV epidemiology, particularly in low-income and lower-middle-income countries.
Funding: EU Innovative Medicines Initiative Preparing for RSV Immunisation and Surveillance in Europe (PROMISE), Bill & Melinda Gates Foundation, and WHO.
© 2024 World Health Organization. Published by Elsevier Ltd. All rights reserved. This is an Open Access article published under the CC BY 3.0 IGO license which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. In any use of this article, there should be no suggestion that WHO endorses any specific organisation, products or services. The use of the WHO logo is not permitted. This notice should be preserved along with the article's original URL.
Conflict of interest statement
Declaration of interests UK is a current employee of Pfizer but took part in this project as a postgraduate student at the University of Edinburgh. NW has received grant funding from the Bill & Melinda Gates Foundation, Sanofi, and US Centers for Disease Control and Prevention. CFY reports grants from the National Medical Research Council Singapore and the Wellcome Trust, and fees from Sanofi, Pfizer, and Takeda, outside of the submitted work. HN reports grants from the Innovative Medicines Initiative related to the submitted work, and grants from WHO, the National Institute for Health Research, Pfizer, and Icosavax, and personal fees from the Bill & Melinda Gates Foundation, Pfizer, ReViral, GlaxoSmithKline, Merck, Icosavax, Sanofi, Novavax, and AbbVie, outside of the submitted work. YL reports grants from WHO, the Wellcome Trust, and GlaxoSmithKline, and personal fees from Pfizer, outside of the submitted work. All other authors declare no competing interests.
Figures
References
-
- Nature Medicine. Progress at last against RSV. Nat Med 2023; 29: 2143. - PubMed
-
- Reyes Domínguez AI, Pavlovic Nesic S, Urquía Martí L, Pérez González MDC, Reyes Suárez D, García-Muñoz Rodrigo F. Effects of public health measures during the SARS-CoV-2 pandemic on the winter respiratory syncytial virus epidemic: an interrupted time series analysis. Paediatr Perinat Epidemiol 2022; 36: 329–36. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
