

Machine learning assisted feature identification and prediction of hemodynamic endpoints using computed tomography in patients with CTEPH
- PMID: 38143250
- PMCID: PMC10950991
- DOI: 10.1007/s10554-023-03026-2
Machine learning assisted feature identification and prediction of hemodynamic endpoints using computed tomography in patients with CTEPH
Abstract
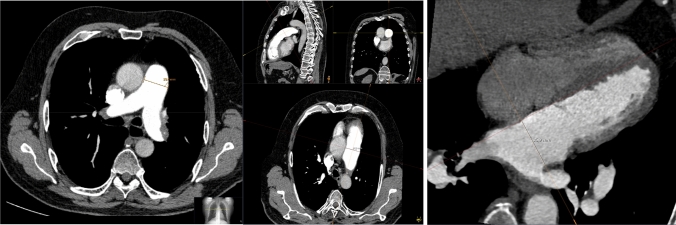
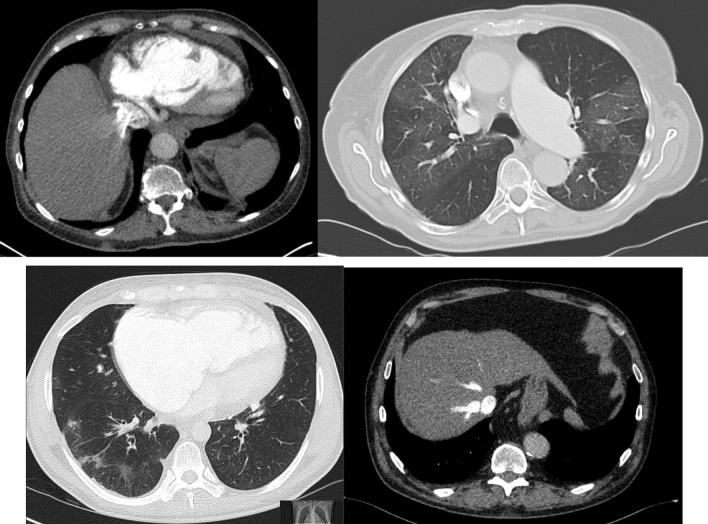
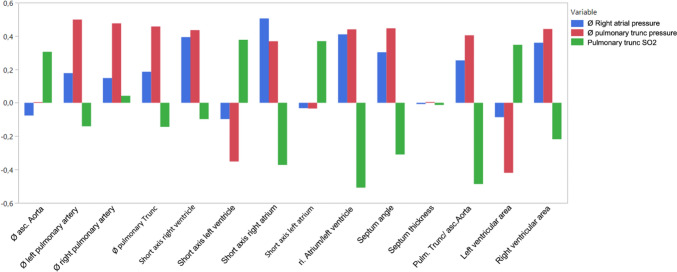
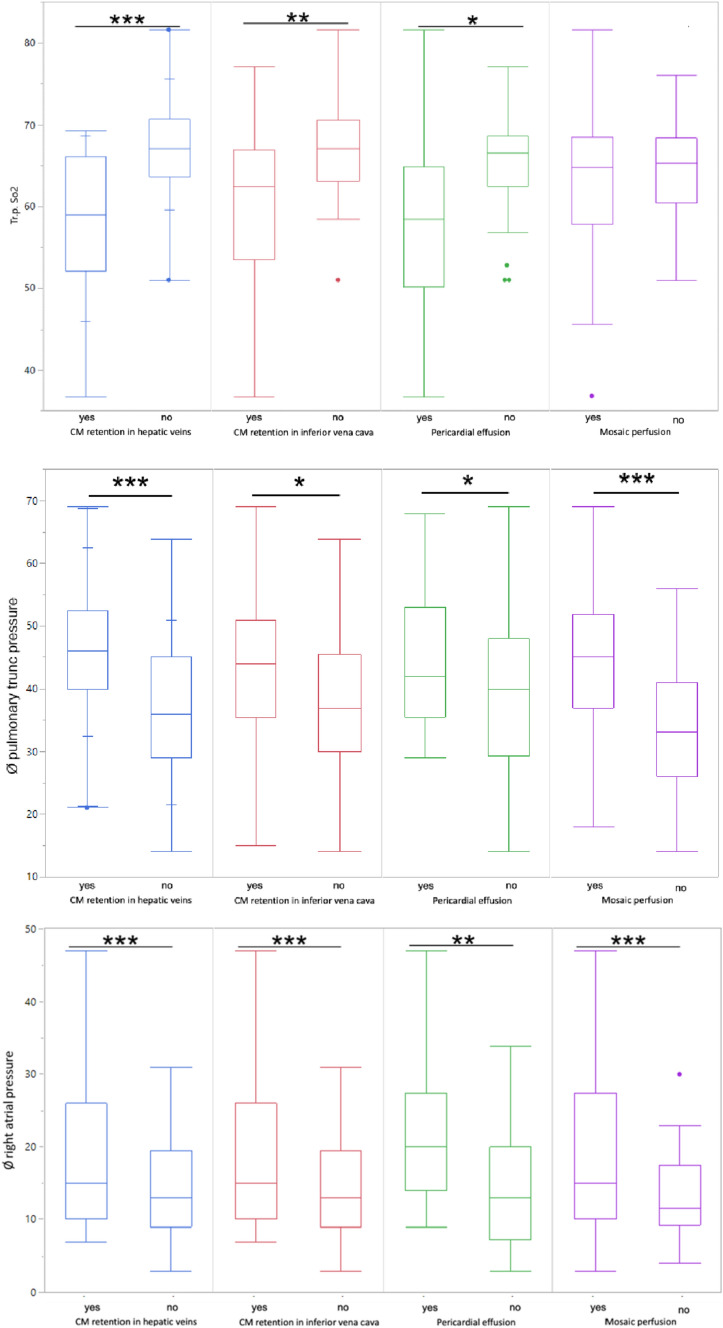
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare but potentially curable cause of pulmonary hypertension (PH). Currently PH is diagnosed by right heart catheterisation. Computed tomography (CT) is used for ruling out other causes and operative planning. This study aims to evaluate importance of different quantitative/qualitative imaging features and develop a supervised machine learning (ML) model to predict hemodynamic risk groups. 127 Patients with diagnosed CTEPH who received preoperative right heart catheterization and thoracic CTA examinations (39 ECG-gated; 88 non-ECG gated) were included. 19 qualitative/quantitative imaging features and 3 hemodynamic parameters [mean pulmonary artery pressure, right atrial pressure (RAP), pulmonary artery oxygen saturation (PA SaO2)] were gathered. Diameter-based CT features were measured in axial and adjusted multiplane reconstructions (MPR). Univariate analysis was performed for qualitative and quantitative features. A random forest algorithm was trained on imaging features to predict hemodynamic risk groups. Feature importance was calculated for all models. Qualitative and quantitative parameters showed no significant differences between ECG and non-ECG gated CTs. Depending on reconstruction plane, five quantitative features were significantly different, but mean absolute difference between parameters (MPR vs. axial) was 0.3 mm with no difference in correlation with hemodynamic parameters. Univariate analysis showed moderate to strong correlation for multiple imaging features with hemodynamic parameters. The model achieved an AUC score of 0.82 for the mPAP based risk stratification and 0.74 for the PA SaO2 risk stratification. Contrast agent retention in hepatic vein, mosaic attenuation pattern and the ratio right atrium/left ventricle were the most important features among other parameters. Quantitative and qualitative imaging features of reconstructions correlate with hemodynamic parameters in preoperative CTEPH patients-regardless of MPR adaption. Machine learning based analysis of preoperative imaging features can be used for non-invasive risk stratification. Qualitative features seem to be more important than previously anticipated.
Keywords: Artificial intelligence; CTEPH; Computed tomography; Pulmonary hypertension.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Vogelmeier CF, Criner GJ, Martinez FJ, Anzueto A, Barnes PJ, Bourbeau J, Celli BR, Chen R, Decramer M, Fabbri LM, Frith P, Halpin DM, Lopez Varela MV, Nishimura M, Roche N, Rodriguez-Roisin R, Sin DD, Singh D, Stockley R, Vestbo J, Wedzicha JA, Agusti A. Global Strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Eur Respir J. 2017;195:557–582. - PubMed
-
- Helmersen D, Provencher S, Hirsch AM, Van Dam A, Dennie C, De Perrot M, Mielniczuk L, Hirani N, Chandy G and Swiston J (2019) Diagnosis of chronic thromboembolic pulmonary hypertension: a Canadian Thoracic Society clinical practice guideline update
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
