

Best Evidence for Each Surgical Step in Minimally Invasive Right Hemicolectomy: A Systematic Review
- PMID: 38144490
- PMCID: PMC10735091
- DOI: 10.1097/AS9.0000000000000343
Best Evidence for Each Surgical Step in Minimally Invasive Right Hemicolectomy: A Systematic Review
Abstract
Objective: The aim of this study was to systematically review the literature for each surgical step of the minimally invasive right hemicolectomy (MIRH) for non-locally advanced colon cancer, to define the most optimal procedure with the highest level of evidence.
Background: High variability exists in the way MIRH is performed between surgeons and hospitals, which could affect patients' postoperative and oncological outcomes.
Methods: A systematic search using PubMed was performed to first identify systematic reviews and meta-analyses, and if there were none then landmark papers and consensus statements were systematically searched for each key step of MIRH. Systematic reviews were assessed using the AMSTAR-2 tool, and selection was based on highest quality followed by year of publication.
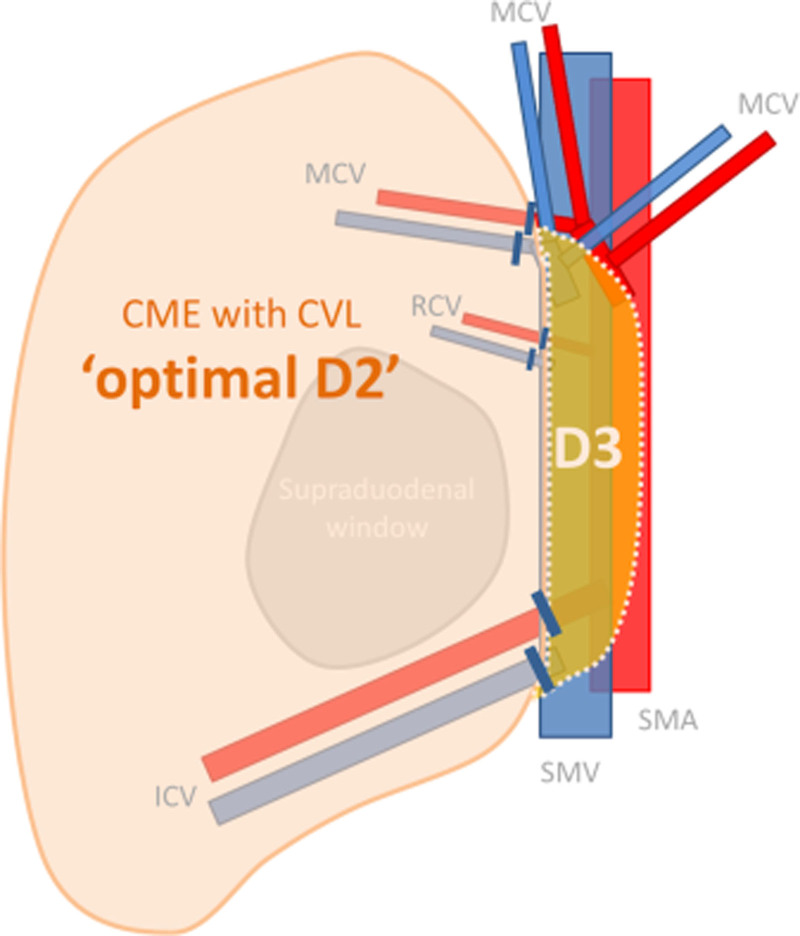
Results: Low (less than 12 mmHg) intra-abdominal pressure (IAP) gives higher mean quality of recovery compared to standard IAP. Complete mesocolic excision (CME) is associated with lowest recurrence and highest 5-year overall survival rates, without worsening short-term outcomes. Routine D3 versus D2 lymphadenectomy showed higher LN yield, but more vascular injuries, and no difference in overall and disease-free survival. Intracorporeal anastomosis is associated with better intra- and postoperative outcomes. The Pfannenstiel incision gives the lowest chance of incisional hernias compared to all other extraction sites.
Conclusion: According to the best available evidence, the most optimal MIRH for colon cancer without clinically involved D3 nodes entails at least low IAP, CME with D2 lymphadenectomy, an intracorporeal anastomosis and specimen extraction through a Pfannenstiel incision.
Keywords: colon cancer; laparoscopic; minimally invasive; right hemicolectomy; right-sided colon cancer; robot-assisted; surgical steps.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Disclosure: The authors declare that they have nothing to disclose.
Figures
References
-
- Aguiar Junior S, Oliveira MM, Silva DRME, et al. . Survival of patients with colorectal cancer in a cancer center. Arq Gastroenterol. 2020;57:172–177. - PubMed
-
- van der Pas MH, Haglind E, Cuesta MA, et al. ; COlorectal cancer Laparoscopic or Open Resection II (COLOR II) Study Group. Laparoscopic versus open surgery for rectal cancer (COLOR II): short-term outcomes of a randomised, phase 3 trial. Lancet Oncol. 2013;14:210–218. - PubMed
-
- Bonjer HJ, Deijen CL, Abis GA, et al. ; COLOR II Study Group. A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med. 2015;372:1324–1332. - PubMed
-
- Jamali FR, Soweid AM, Dimassi H, et al. . Evaluating the degree of difficulty of laparoscopic colorectal surgery. Arch Surg. 2008;143:762–7; discussion 768. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
