

Identifying brain tumor patients' subtypes based on pre-diagnostic history and clinical characteristics: a pilot hierarchical clustering and association analysis
- PMID: 38146510
- PMCID: PMC10749422
- DOI: 10.3389/fonc.2023.1276253
Identifying brain tumor patients' subtypes based on pre-diagnostic history and clinical characteristics: a pilot hierarchical clustering and association analysis
Abstract
Introduction: Central nervous system (CNS) tumors are severe health conditions with increasing incidence in the last years. Different biological, environmental and clinical factors are thought to have an important role in their epidemiology, which however remains unclear.
Objective: The aim of this pilot study was to identify CNS tumor patients' subtypes based on this information and to test associations with tumor malignancy.
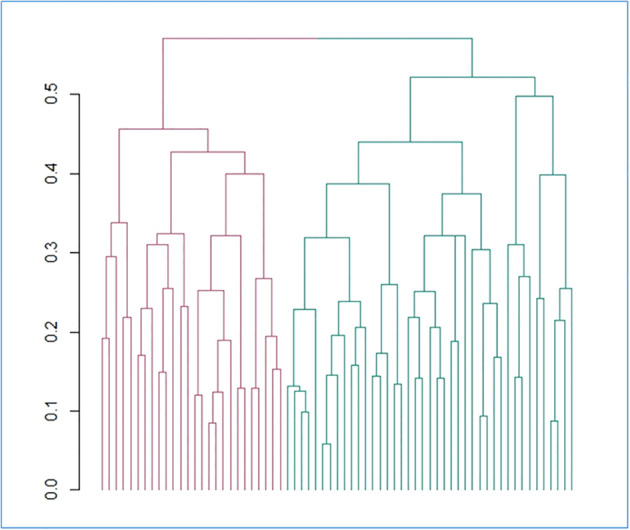
Methods: 90 patients with suspected diagnosis of CNS tumor were recruited by the Neurosurgery Unit of IRCCS Neuromed. Patients underwent anamnestic and clinical assessment, to ascertain known or suspected risk factors including lifestyle, socioeconomic, clinical and psychometric characteristics. We applied a hierarchical clustering analysis to these exposures to identify potential groups of patients with a similar risk pattern and tested whether these clusters associated with brain tumor malignancy.
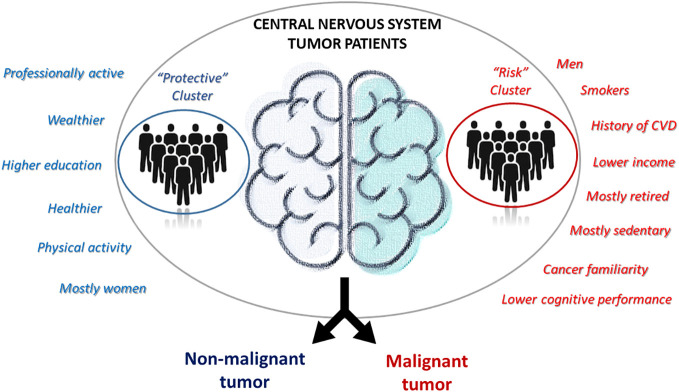
Results: Out of 67 patients with a confirmed CNS tumor diagnosis, we identified 28 non-malignant and 39 malignant tumor cases. These subtypes showed significant differences in terms of gender (with men more frequently presenting a diagnosis of cancer; p = 6.0 ×10-3) and yearly household income (with non-malignant tumor patients more frequently earning ≥25k Euros/year; p = 3.4×10-3). Cluster analysis revealed the presence of two clusters of patients: one (N=41) with more professionally active, educated, wealthier and healthier patients, and the other one with mostly retired and less healthy men, with a higher frequency of smokers, personal history of cardiovascular disease and cancer familiarity, a mostly sedentary lifestyle and generally lower income, education and cognitive performance. The former cluster showed a protective association with the malignancy of the disease, with a 74 (14-93) % reduction in the prevalent risk of CNS malignant tumors, compared to the other cluster (p=0.026).
Discussion: These preliminary data suggest that patients' profiling through unsupervised machine learning approaches may somehow help predicting the risk of being affected by a malignant form. If confirmed by further analyses in larger independent cohorts, these findings may be useful to create potential intelligent ranking systems for treatment priority, overcoming the lack of histopathological information and molecular diagnosis of the tumor, which are typically not available until the time of surgery.
Keywords: cancer diagnosis; central nervous system tumors; clinical characteristics; cluster analysis; cognitive performance; malignancy; pre-diagnostic history; risk and protective factors.
Copyright © 2023 Esposito, Ruggiero, Di Castelnuovo, Costanzo, Bonaccio, Bracone, Esposito, Innocenzi, Paolini, Cerletti, Donati, de Gaetano, Iacoviello and Gialluisi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that ER was a review editor, MB, MD, GdG and LI were all Guest associate editors, VE was an associate editor and AG was a Guest Associate Editor and Review Editor and they were all members of the Frontiers, editorial board member of at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Mortality and Morbidity Effects of Long-Term Exposure to Low-Level PM2.5, BC, NO2, and O3: An Analysis of European Cohorts in the ELAPSE Project.Res Rep Health Eff Inst. 2021 Sep;2021(208):1-127. Res Rep Health Eff Inst. 2021. PMID: 36106702 Free PMC article.
-
Letter to the Editor: Depression As The First Symptom Of Frontal Lobe Grade 2 Malignant Glioma.Turk Psikiyatri Derg. 2022 Summer;33(2):143-145. doi: 10.5080/u25957. Turk Psikiyatri Derg. 2022. PMID: 35730515 English, Turkish.
-
Challenges of Clustering Multimodal Clinical Data: Review of Applications in Asthma Subtyping.JMIR Med Inform. 2020 May 28;8(5):e16452. doi: 10.2196/16452. JMIR Med Inform. 2020. PMID: 32463370 Free PMC article. Review.
-
Italian cancer figures, report 2012: Cancer in children and adolescents.Epidemiol Prev. 2013 Jan-Feb;37(1 Suppl 1):1-225. Epidemiol Prev. 2013. PMID: 23585445 English, Italian.
-
Peritonsillar abscess: clinical aspects of microbiology, risk factors, and the association with parapharyngeal abscess.Dan Med J. 2017 Mar;64(3):B5333. Dan Med J. 2017. PMID: 28260599 Review.
References
LinkOut - more resources
Full Text Sources